
Page 6 - Veritax EE Guide 10-1-2019 - CA
P. 6
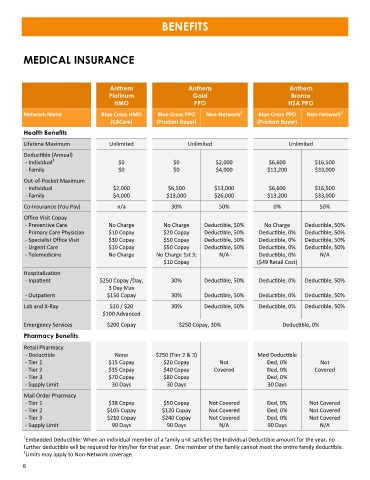
BENEFITS
MEDICAL INSURANCE
Anthem Anthem Anthem
Platinum Gold Bronze
HMO PPO HSA PPO
2
2
Network Name Blue Cross HMO Blue Cross PPO Non-Network Blue Cross PPO Non-Network
(CACare) (Prudent Buyer) (Prudent Buyer)
Health Benefits
Lifetime Maximum Unlimited Unlimited Unlimited
Deductible (Annual)
1
- Individual $0 $0 $2,000 $6,600 $16,500
- Family $0 $0 $4,000 $13,200 $33,000
Out-of-Pocket Maximum
- Individual $2,000 $6,500 $13,000 $6,600 $16,500
- Family $4,000 $13,000 $26,000 $13,200 $33,000
Co-Insurance (You Pay) n/a 30% 50% 0% 50%
Office Visit Copay
- Preventive Care No Charge No Charge Deductible, 50% No Charge Deductible, 50%
- Primary Care Physician $10 Copay $20 Copay Deductible, 50% Deductible, 0% Deductible, 50%
- Specialist Office Visit $30 Copay $50 Copay Deductible, 50% Deductible, 0% Deductible, 50%
- Urgent Care $10 Copay $50 Copay Deductible, 50% Deductible, 0% Deductible, 50%
- Telemedicine No Charge No Charge 1st 3; N/A Deductible, 0% N/A
$10 Copay ($49 Retail Cost)
Hospitalization
- Inpatient $250 Copay /Day, 30% Deductible, 50% Deductible, 0% Deductible, 50%
3 Day Max
- Outpatient $150 Copay 30% Deductible, 50% Deductible, 0% Deductible, 50%
Lab and X-Ray $10 / $20 30% Deductible, 50% Deductible, 0% Deductible, 50%
$100 Advanced
Emergency Services $200 Copay $250 Copay, 30% Deductible, 0%
Pharmacy Benefits
Retail Pharmacy
- Deductible None $250 (Tier 2 & 3) Med Deductible
- Tier 1 $15 Copay $20 Copay Not Ded, 0% Not
- Tier 2 $35 Copay $40 Copay Covered Ded, 0% Covered
- Tier 3 $70 Copay $80 Copay Ded, 0%
- Supply Limit 30 Days 30 Days 30 Days
Mail Order Pharmacy
- Tier 1 $38 Copay $50 Copay Not Covered Ded, 0% Not Covered
- Tier 2 $105 Copay $120 Copay Not Covered Ded, 0% Not Covered
- Tier 3 $210 Copay $240 Copay Not Covered Ded, 0% Not Covered
- Supply Limit 90 Days 90 Days N/A 90 Days N/A
1
Embedded Deductible: When an individual member of a family unit satisfies the Individual Deductible amount for the year, no
further deductible will be required for him/her for that year. One member of the family cannot meet the entire family deductible.
2
Limits may apply to Non-Network coverage.
6