
Page 6 - FINAL Crane Country Day School 2017-18 Benefits Guide
P. 6
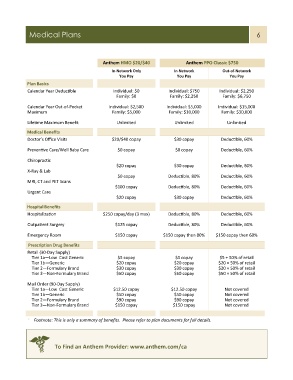
Medical Plans 6
Anthem HMO $20/$40 Anthem PPO Classic $750
In-Network Only In-Network Out-of-Network
You Pay You Pay You Pay
Plan Basics
Calendar Year Deductible Individual: $0 Individual: $750 Individual: $2,250
Family: $0 Family: $2,250 Family: $6,750
Calendar Year Out-of-Pocket Individual: $2,500 Individual: $5,000 Individual: $15,000
Maximum Family: $5,000 Family: $10,000 Family: $30,000
Lifetime Maximum Benefit Unlimited Unlimited Unlimited
Medical Benefits
Doctor’s Office Visits $20/$40 copay $30 copay Deductible, 60%
Preventive Care/Well Baby Care $0 copay $0 copay Deductible, 60%
Chiropractic
$20 copay $30 copay Deductible, 60%
X-Ray & Lab
$0 copay Deductible, 80% Deductible, 60%
MRI, CT and PET Scans
$100 copay Deductible, 80% Deductible, 60%
Urgent Care
$20 copay $30 copay Deductible, 60%
Hospital Benefits
Hospitalization $250 copay/day (3 max) Deductible, 80% Deductible, 60%
Outpatient Surgery $125 copay Deductible, 80% Deductible, 60%
Emergency Room $150 copay $150 copay then 80% $150 copay then 60%
Prescription Drug Benefits
Retail (30-Day Supply)
Tier 1a—Low Cost Generic $5 copay $5 copay $5 + 50% of retail
Tier 1b—Generic $20 copay $20 copay $20 + 50% of retail
Tier 2—Formulary Brand $30 copay $30 copay $20 + 50% of retail
Tier 3—Non-Formulary Brand $50 copay $50 copay $50 + 50% of retail
Mail Order (90-Day Supply)
Tier 1a—Low Cost Generic $12.50 copay $12.50 copay Not covered
Tier 1b—Generic $50 copay $50 copay Not covered
Tier 2—Formulary Brand $90 copay $90 copay Not covered
Tier 3—Non-Formulary Brand $150 copay $150 copay Not covered
* Footnote: This is only a summary of benefits. Please refer to plan documents for full details.
To Find an Anthem Provider: www.anthem.com/ca