
Page 6 - Veritone's EE Guide final
P. 6
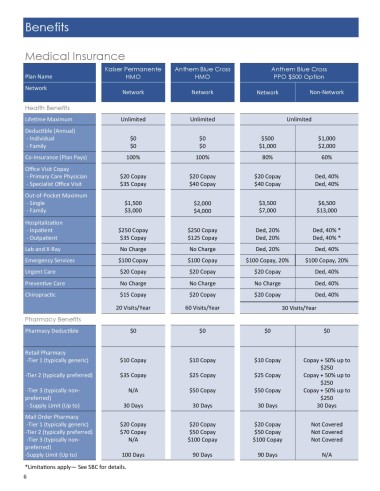
Benefits
Medical Insurance
Kaiser Permanente Anthem Blue Cross Anthem Blue Cross
Plan Name HMO HMO PPO $500 Option
Network
Network Network Network Non-Network
Health Benefits
Lifetime Maximum Unlimited Unlimited Unlimited
Deductible (Annual)
- Individual $0 $0 $500 $1,000
- Family $0 $0 $1,000 $2,000
Co-Insurance (Plan Pays) 100% 100% 80% 60%
Office Visit Copay
- Primary Care Physician $20 Copay $20 Copay $20 Copay Ded, 40%
- Specialist Office Visit $35 Copay $40 Copay $40 Copay Ded, 40%
Out-of-Pocket Maximum
- Single $1,500 $2,000 $3,500 $6,500
- Family $3,000 $4,000 $7,000 $13,000
Hospitalization
- Inpatient $250 Copay $250 Copay Ded, 20% Ded, 40% *
- Outpatient $35 Copay $125 Copay Ded, 20% Ded, 40% *
Lab and X-Ray No Charge No Charge Ded, 20% Ded, 40%
Emergency Services $100 Copay $100 Copay $100 Copay, 20% $100 Copay, 20%
Urgent Care $20 Copay $20 Copay $20 Copay Ded, 40%
Preventive Care No Charge No Charge No Charge Ded, 40%
Chiropractic $15 Copay $20 Copay $20 Copay Ded, 40%
20 Visits/Year 60 Visits/Year 30 Visits/Year
Pharmacy Benefits
Pharmacy Deductible $0 $0 $0 $0
Retail Pharmacy
-Tier 1 (typically generic) $10 Copay $10 Copay $10 Copay Copay + 50% up to
$250
-Tier 2 (typically preferred) $35 Copay $25 Copay $25 Copay Copay + 50% up to
$250
-Tier 3 (typically non- N/A $50 Copay $50 Copay Copay + 50% up to
preferred) $250
- Supply Limit (Up to) 30 Days 30 Days 30 Days 30 Days
Mail Order Pharmacy
-Tier 1 (typically generic) $20 Copay $20 Copay $20 Copay Not Covered
-Tier 2 (typically preferred) $70 Copay $50 Copay $50 Copay Not Covered
-Tier 3 (typically non- N/A $100 Copay $100 Copay Not Covered
preferred)
-Supply Limit (Up to) 100 Days 90 Days 90 Days N/A
*Limitations apply— See SBC for details.
6