
Page 6 - Kagan Benefit Guide CA.pub
P. 6
Benefits
Dental Insurance
Principal | POS Dental Plan
With the Principal Point of Service (POS) dental plan, you may visit an EPO or PPO den st and benefit from the nego ated rate or
visit a non‐network den st. With Point of Service, the benefit received is determined at the me of service depending on the type
of provider you visit for care. A Point of Service design incorporates three benefit levels – Exclusive Provider Organiza on (EPO),
Preferred Provider Organiza on (PPO) and non‐network. You receive greater savings through den sts who par cipate in the EPO
and PPO networks. You may also obtain services using a non‐network dentist; however, you will be responsible for the difference
between the covered amount and the actual charges and you may be responsible for filing claims.
Principal | EPO Dental Plan
With the Exclusive Provider Organiza on (EPO) plan through Principal, you may visit an EPO den st and benefit from the
nego ated rates for covered services. Out of network services are not covered under this plan.
Note
We strongly recommend you ask your den st for a predetermina on if total charges are
expected to exceed $300. Predetermina on enables you and your den st to know in ad‐
vance what the payment will be for any service that may be in ques on.
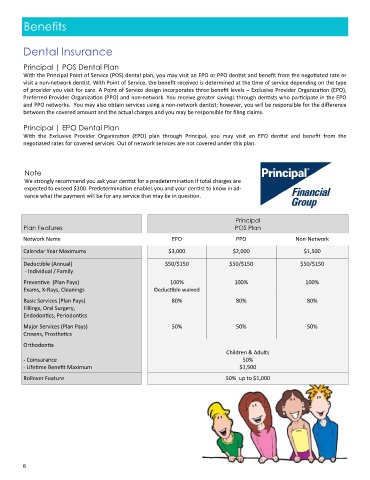
Principal
Plan Features POS Plan
Network Name EPO PPO Non‐Network
Calendar Year Maximums $3,000 $2,000 $1,500
Deduc ble (Annual) $50/$150 $50/$150 $50/$150
‐ Individual / Family
Preven ve (Plan Pays) 100% 100% 100%
Exams, X‐Rays, Cleanings Deduc ble waived
Basic Services (Plan Pays) 80% 80% 80%
Fillings, Oral Surgery,
Endodon cs, Periodon cs
Major Services (Plan Pays) 50% 50% 50%
Crowns, Prosthe cs
Orthodon a
Children & Adults
‐ Coinsurance 50%
‐ Life me Benefit Maximum $1,500
Rollover Feature 50% up to $1,000
6