
Page 7 - Benefits Guide BICS 2020 Final
P. 7
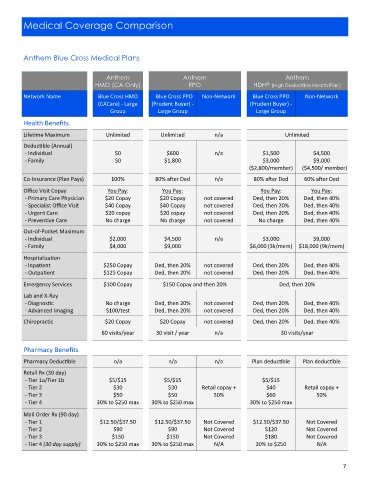
Medical Coverage Comparison
Anthem Blue Cross Medical Plans
Anthem Anthem Anthem
HMO (CA Only) EPO HDHP (High Deductible Health Plan)
Network Name Blue Cross HMO Blue Cross PPO Non-Network Blue Cross PPO Non-Network
(CACare) - Large (Prudent Buyer) - (Prudent Buyer) -
Group Large Group Large Group
Health Benefits
Lifetime Maximum Unlimited Unlimited n/a Unlimited
Deductible (Annual)
- Individual $0 $600 n/a $1,500 $4,500
- Family $0 $1,800 $3,000 $9,000
($2,800/member) ($4,500/ member)
Co-Insurance (Plan Pays) 100% 80% after Ded n/a 80% after Ded 60% after Ded
Office Visit Copay You Pay: You Pay: You Pay: You Pay:
- Primary Care Physician $20 Copay $20 Copay not covered Ded, then 20% Ded, then 40%
- Specialist Office Visit $40 Copay $40 Copay not covered Ded, then 20% Ded, then 40%
- Urgent Care $20 copay $20 copay not covered Ded, then 20% Ded, then 40%
- Preventive Care No charge No charge not covered No charge Ded, then 40%
Out-of-Pocket Maximum
- Individual $2,000 $4,500 n/a $3,000 $9,000
- Family $4,000 $9,000 $6,000 (3k/mem) $18,000 (9k/mem)
Hospitalization
- Inpatient $250 Copay Ded, then 20% not covered Ded, then 20% Ded, then 40%
- Outpatient $125 Copay Ded, then 20% not covered Ded, then 20% Ded, then 40%
Emergency Services $100 Copay $150 Copay and then 20% Ded, then 20%
Lab and X-Ray
- Diagnostic No charge Ded, then 20% not covered Ded, then 20% Ded, then 40%
- Advanced Imaging $100/test Ded, then 20% not covered Ded, then 20% Ded, then 40%
Chiropractic $20 Copay $20 Copay not covered Ded, then 20% Ded, then 40%
60 visits/year 30 visit / year n/a 30 visits/year
Pharmacy Benefits
Pharmacy Deductible n/a n/a n/a Plan deductible Plan deductible
Retail Rx (30 day)
- Tier 1a/Tier 1b $5/$15 $5/$15 $5/$15
- Tier 2 $30 $30 Retail copay + $40 Retail copay +
- Tier 3 $50 $50 50% $60 50%
- Tier 4 30% to $250 max 30% to $250 max 30% to $250 max
Mail Order Rx (90 day)
- Tier 1 $12.50/$37.50 $12.50/$37.50 Not Covered $12.50/$37.50 Not Covered
- Tier 2 $90 $90 Not Covered $120 Not Covered
- Tier 3 $150 $150 Not Covered $180 Not Covered
- Tier 4 (30 day supply) 30% to $250 max 30% to $250 max N/A 30% to $250 N/A
7