
Page 7 - California Eye Management EE Guide 2020
P. 7
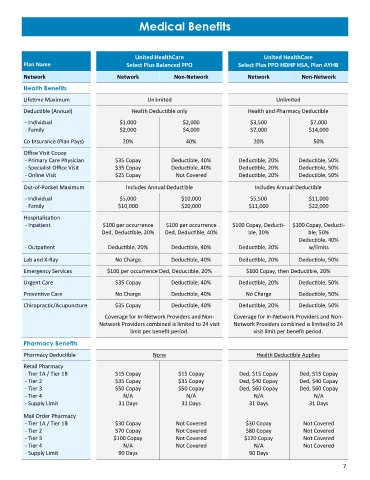
Medical Benefits
United HealthCare United HealthCare
Plan Name Select Plus Balanced PPO Select Plus PPO HDHP HSA, Plan AYHB
Network Network Non-Network Network Non-Network
Health Benefits
Lifetime Maximum Unlimited Unlimited
Deductible (Annual) Health Deductible only Health and Pharmacy Deductible
- Individual $1,000 $2,000 $3,500 $7,000
- Family $2,000 $4,000 $7,000 $14,000
Co-Insurance (Plan Pays) 20% 40% 20% 50%
Office Visit Copay
- Primary Care Physician $35 Copay Deductible, 40% Deductible, 20% Deductible, 50%
- Specialist Office Visit $35 Copay Deductible, 40% Deductible, 20% Deductible, 50%
- Online Visit $25 Copay Not Covered Deductible, 20% Deductible, 50%
Out-of-Pocket Maximum Includes Annual Deductible Includes Annual Deductible
- Individual $5,000 $10,000 $5,500 $11,000
- Family $10,000 $20,000 $11,000 $22,000
Hospitalization
- Inpatient $100 per occurrence $100 per occurrence $100 Copay, Deducti- $100 Copay, Deducti-
Ded, Deductible, 20% Ded, Deductible, 40% ble, 20% ble, 50%
Deductible, 40%
- Outpatient Deductible, 20% Deductible, 40% Deductible, 20% w/limits
Lab and X-Ray No Charge Deductible, 40% Deductible, 20% Deductible, 50%
Emergency Services $100 per occurrence Ded, Deductible, 20% $100 Copay, then Deductible, 20%
Urgent Care $35 Copay Deductible, 40% Deductible, 20% Deductible, 50%
Preventive Care No Charge Deductible, 40% No Charge Deductible, 50%
Chiropractic/Acupuncture $35 Copay Deductible, 40% Deductible, 20% Deductible, 50%
Coverage for In-Network Providers and Non- Coverage for In-Network Providers and Non-
Network Providers combined is limited to 24 visit Network Providers combined is limited to 24
limit per benefit period. visit limit per benefit period.
Pharmacy Benefits
Pharmacy Deductible None Health Deductible Applies
Retail Pharmacy
- Tier 1A / Tier 1B $15 Copay $15 Copay Ded, $15 Copay Ded, $15 Copay
- Tier 2 $35 Copay $35 Copay Ded, $40 Copay Ded, $40 Copay
- Tier 3 $50 Copay $50 Copay Ded, $60 Copay Ded, $60 Copay
- Tier 4 N/A N/A N/A N/A
- Supply Limit 31 Days 31 Days 31 Days 31 Days
Mail Order Pharmacy
- Tier 1A / Tier 1B $30 Copay Not Covered $30 Copay Not Covered
- Tier 2 $70 Copay Not Covered $80 Copay Not Covered
- Tier 3 $100 Copay Not Covered $120 Copay Not Covered
- Tier 4 N/A Not Covered N/A Not Covered
- Supply Limit 90 Days 90 Days
7