
Page 8 - Sumitomo EE Guide 06-20 Final English
P. 8
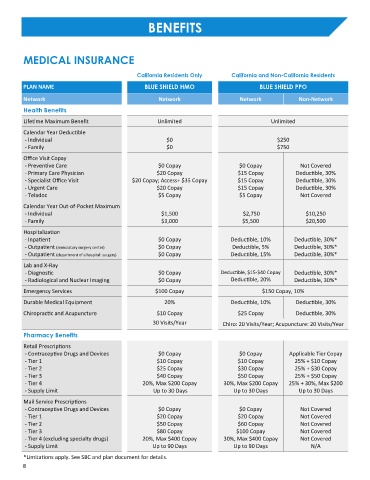
BENEFITS
MEDICAL INSURANCE
California Residents Only California and Non-California Residents
PLAN NAME BLUE SHIELD HMO BLUE SHIELD PPO
Network Network Network Non-Network
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited
Calendar Year Deductible
- Individual $0 $250
- Family $0 $750
Office Visit Copay
- Preventive Care $0 Copay $0 Copay Not Covered
- Primary Care Physician $20 Copay $15 Copay Deductible, 30%
- Specialist Office Visit $20 Copay; Access+ $35 Copay $15 Copay Deductible, 30%
- Urgent Care $20 Copay $15 Copay Deductible, 30%
- Teladoc $5 Copay $5 Copay Not Covered
Calendar Year Out-of-Pocket Maximum
- Individual $1,500 $2,750 $10,250
- Family $3,000 $5,500 $20,500
Hospitalization
- Inpatient $0 Copay Deductible, 10% Deductible, 30%*
- Outpatient (ambulatory surgery center) $0 Copay Deductible, 5% Deductible, 30%*
- Outpatient (department of a hospital: surgery) $0 Copay Deductible, 15% Deductible, 30%*
Lab and X-Ray
- Diagnostic $0 Copay Deductible, $15-$40 Copay Deductible, 30%*
- Radiological and Nuclear Imaging $0 Copay Deductible, 20% Deductible, 30%*
Emergency Services $100 Copay $150 Copay, 10%
Durable Medical Equipment 20% Deductible, 10% Deductible, 30%
Chiropractic and Acupuncture $10 Copay $25 Copay Deductible, 30%
30 Visits/Year Chiro: 20 Visits/Year; Acupuncture: 20 Visits/Year
Pharmacy Benefits
Retail Prescriptions
- Contraceptive Drugs and Devices $0 Copay $0 Copay Applicable Tier Copay
- Tier 1 $10 Copay $10 Copay 25% + $10 Copay
- Tier 2 $25 Copay $30 Copay 25% + $30 Copay
- Tier 3 $40 Copay $50 Copay 25% + $50 Copay
- Tier 4 20%, Max $200 Copay 30%, Max $200 Copay 25% + 30%, Max $200
- Supply Limit Up to 30 Days Up to 30 Days Up to 30 Days
Mail Service Prescriptions
- Contraceptive Drugs and Devices $0 Copay $0 Copay Not Covered
- Tier 1 $20 Copay $20 Copay Not Covered
- Tier 2 $50 Copay $60 Copay Not Covered
- Tier 3 $80 Copay $100 Copay Not Covered
- Tier 4 (excluding specialty drugs) 20%, Max $400 Copay 30%, Max $400 Copay Not Covered
- Supply Limit Up to 90 Days Up to 90 Days N/A
*Limitations apply. See SBC and plan document for details.
8