
Page 7 - UP_Benefits_2018_NonCA_Support_110917_FLIP
P. 7
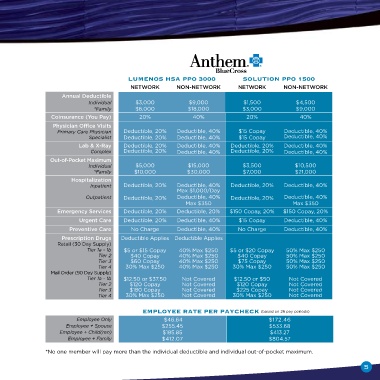
EnrollmEnt InformatIon
luMEnoS hSa PPo 3000 Solution PPo 1500
neTwoRk non-neTwoRk neTwoRk non-neTwoRk
Annual Deductible
Individual $3,000 $9,000 $1,500 $4,500
*Family $6,000 $18,000 $3,000 $9,000
Coinsurance (You Pay) 20% 40% 20% 40%
Physician office Visits
Primary Care Physician Deductible, 20% Deductible, 40% $15 Copay Deductible, 40%
Specialist Deductible, 20% Deductible, 40% $15 Copay Deductible, 40%
Lab & X-Ray Deductible, 20% Deductible, 40% Deductible, 20% Deductible, 40%
Complex Deductible, 20% Deductible, 40% Deductible, 20% Deductible, 40%
out-of-Pocket Maximum
Individual $5,000 $15,000 $3,500 $10,500
*Family $10,000 $30,000 $7,000 $21,000
Hospitalization
Inpatient Deductible, 20% Deductible, 40% Deductible, 20% Deductible, 40%
Max $1,000/Day
Outpatient Deductible, 20% Deductible, 40% Deductible, 20% Deductible, 40%
Max $350 Max $350
emergency Services Deductible, 20% Deductible, 20% $150 Copay, 20% $150 Copay, 20%
Urgent Care Deductible, 20% Deductible, 40% $15 Copay Deductible, 40%
Preventive Care No Charge Deductible, 40% No Charge Deductible, 40%
Prescription Drugs Deductible Applies Deductible Applies
Retail (30 Day Supply)
Tier 1a - 1b $5 or $15 Copay 40% Max $250 $5 or $20 Copay 50% Max $250
Tier 2 $40 Copay 40% Max $250 $40 Copay 50% Max $250
Tier 3 $60 Copay 40% Max $250 $75 Copay 50% Max $250
Tier 4 30% Max $250 40% Max $250 30% Max $250 50% Max $250
Mail Order (90 Day Supply)
Tier 1a - 1b $12.50 or $37.50 Not Covered $12.50 or $50 Not Covered
Tier 2 $120 Copay Not Covered $120 Copay Not Covered
Tier 3 $180 Copay Not Covered $225 Copay Not Covered
Tier 4 30% Max $250 Not Covered 30% Max $250 Not Covered
EMPloyEE ratE PEr PayChECk (based on 26 pay periods)
Employee Only $46.64 $172.46
Employee + Spouse $255.45 $533.68
Employee + Child(ren) $185.85 $413.27
Employee + Family $412.07 $804.57
*No one member will pay more than the individual deductible and individual out-of-pocket maximum.
5