
Page 19 - open_enrollment_benefits_book_NA_2018_v4
P. 19
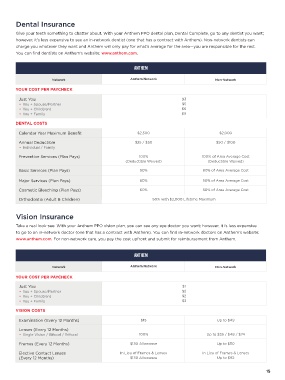
Dental Insurance
Give your teeth something to chatter about. With your Anthem PPO dental plan, Dental Complete, go to any dentist you want;
however, it’s less expensive to see an in-network dentist (one that has a contract with Anthem). Non-network dentists can
charge you whatever they want and Anthem will only pay for what’s average for the area—you are responsible for the rest.
You can find dentists on Anthem’s website: www.anthem.com.
ANTHEM
Network Anthem Network Non-Network
YOUR COST PER PAYCHECK
Just You $3
• You + Spouse/Partner $5
• You + Child(ren) $6
• You + Family $9
DENTAL COSTS
Calendar Year Maximum Benefit $2,500 $2,000
Annual Deductible $25 / $50 $50 / $100
• Individual / Family
Preventive Services (Plan Pays) 100% 100% of Area Average Cost
(Deductible Waived) (Deductible Waived)
Basic Services (Plan Pays) 90% 80% of Area Average Cost
Major Services (Plan Pays) 60% 50% of Area Average Cost
Cosmetic Bleaching (Plan Pays) 60% 50% of Area Average Cost
Orthodontia (Adult & Children) 50% with $2,000 Lifetime Maximum
Vision Insurance
Take a real look-see. With your Anthem PPO vision plan, you can see any eye doctor you want; however, it is less expensive
to go to an in-network doctor (one that has a contract with Anthem). You can find in-network doctors on Anthem’s website:
www.anthem.com. For non-network care, you pay the cost upfront and submit for reimbursement from Anthem.
ANTHEM
Network Anthem Network Non-Network
YOUR COST PER PAYCHECK
Just You $1
• You + Spouse/Partner $2
• You + Child(ren) $2
• You + Family $3
VISION COSTS
Examination (Every 12 Months) $15 Up to $49
Lenses (Every 12 Months)
• Single Vision / Bifocal / Trifocal 100% Up to $35 / $49 / $74
Frames (Every 12 Months) $130 Allowance Up to $50
Elective Contact Lenses In Lieu of Frames & Lenses In Lieu of Frames & Lenses
(Every 12 Months) $130 Allowance Up to $92
15