
Page 8 - Wellbiz Brands Benefit Guide 2020
P. 8
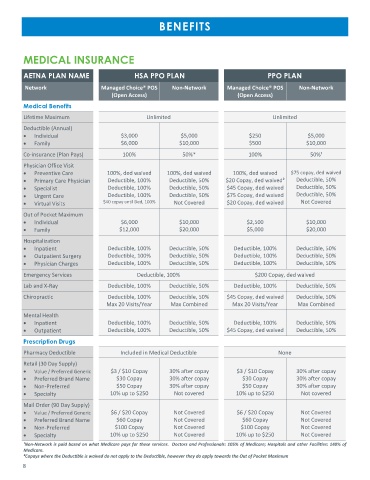
BENEFITS
MEDICAL INSURANCE
AETNA PLAN NAME HSA PPO PLAN PPO PLAN
Network Managed Choice® POS Non-Network Managed Choice® POS Non-Network
(Open Access) (Open Access)
Medical Benefits
Lifetime Maximum Unlimited Unlimited
Deductible (Annual)
• Individual $3,000 $5,000 $250 $5,000
• Family $6,000 $10,000 $500 $10,000
Co-insurance (Plan Pays) 100% 50%* 100% 50%¹
Physician Office Visit
• Preventive Care 100%, ded waived 100%, ded waived 100%, ded waived $75 copay, ded waived
• Primary Care Physician Deductible, 100% Deductible, 50% $20 Copay, ded waived² Deductible, 50%
• Specialist Deductible, 100% Deductible, 50% $45 Copay, ded waived Deductible, 50%
• Urgent Care Deductible, 100% Deductible, 50% $75 Copay, ded waived Deductible, 50%
• Virtual Visits $40 copay until Ded, 100% Not Covered $20 Copay, ded waived Not Covered
Out of Pocket Maximum
• Individual $6,000 $10,000 $2,500 $10,000
• Family $12,000 $20,000 $5,000 $20,000
Hospitalization
• Inpatient Deductible, 100% Deductible, 50% Deductible, 100% Deductible, 50%
• Outpatient Surgery Deductible, 100% Deductible, 50% Deductible, 100% Deductible, 50%
• Physician Charges Deductible, 100% Deductible, 50% Deductible, 100% Deductible, 50%
Emergency Services Deductible, 100% $200 Copay, ded waived
Lab and X-Ray Deductible, 100% Deductible, 50% Deductible, 100% Deductible, 50%
Chiropractic Deductible, 100% Deductible, 50% $45 Copay, ded waived Deductible, 50%
Max 20 Visits/Year Max Combined Max 20 Visits/Year Max Combined
Mental Health
• Inpatient Deductible, 100% Deductible, 50% Deductible, 100% Deductible, 50%
• Outpatient Deductible, 100% Deductible, 50% $45 Copay, ded waived Deductible, 50%
Prescription Drugs
Pharmacy Deductible Included in Medical Deductible None
Retail (30 Day Supply)
• Value / Preferred Generic $3 / $10 Copay 30% after copay $3 / $10 Copay 30% after copay
• Preferred Brand Name $30 Copay 30% after copay $30 Copay 30% after copay
• Non-Preferred $50 Copay 30% after copay $50 Copay 30% after copay
• Specialty 10% up to $250 Not covered 10% up to $250 Not covered
Mail Order (90 Day Supply)
• Value / Preferred Generic $6 / $20 Copay Not Covered $6 / $20 Copay Not Covered
• Preferred Brand Name $60 Copay Not Covered $60 Copay Not Covered
• Non-Preferred $100 Copay Not Covered $100 Copay Not Covered
• Specialty 10% up to $250 Not Covered 10% up to $250 Not Covered
¹Non-Network is paid based on what Medicare pays for these services. Doctors and Professionals: 105% of Medicare; Hospitals and other Facilities: 140% of
Medicare.
²Copays where the Deductible is waived do not apply to the Deductible, however they do apply towards the Out of Pocket Maximum
8