
Page 45 - New Hire Kit (Non-Union)
P. 45
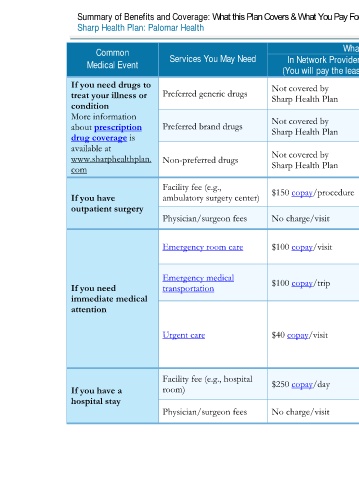
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2020 – 12/31/2020
Sharp Health Plan: Palomar Health Coverage for: Individual / Family | Plan Type: HDHP HMO
Common Services You May Need What You Will Pay Limitations, Exceptions, & Other Important
Medical Event In Network Provider Out-of-Network Provider Information
(You will pay the least) (You will pay the most)
If you need drugs to Not covered by Not covered by
treat your illness or Preferred generic drugs Sharp Health Plan Sharp Health Plan
condition
More information Not covered by Not covered by Administered by CVS Caremark
about prescription Preferred brand drugs Sharp Health Plan Sharp Health Plan 800-776-1355 / Caremark.com
drug coverage is
available at
www.sharphealthplan. Non-preferred drugs Not covered by Not covered by
com Sharp Health Plan Sharp Health Plan
Facility fee (e.g., Not covered
If you have ambulatory surgery center) $150 copay/procedure Preauthorization is required.
outpatient surgery
Physician/surgeon fees No charge/visit Not covered
Cost sharing waived if admitted to the
Emergency room care $100 copay/visit $100 copay/visit
hospital.
Emergency medical
If you need transportation $100 copay/trip $100 copay/trip None
immediate medical
attention Services must be approved by your primary
care provider and received at urgent care
facilities affiliated with your Plan Medical
Urgent care $40 copay/visit $40 copay/visit
Group. Out-of-Network services are covered
only when you are outside of the Service Area
for your Plan Network.
Facility fee (e.g., hospital $250 copay/day $250 copay/day
If you have a room) Preauthorization is required for non-
hospital stay emergency services. Out-of-network services
are covered for emergency care only.
Physician/surgeon fees No charge/visit No charge/visit
3 of 11
Palomar Health HMO NG 2 L / ACCH15_40 / VSA8