
Page 47 - New Hire Kit (Non-Union)
P. 47
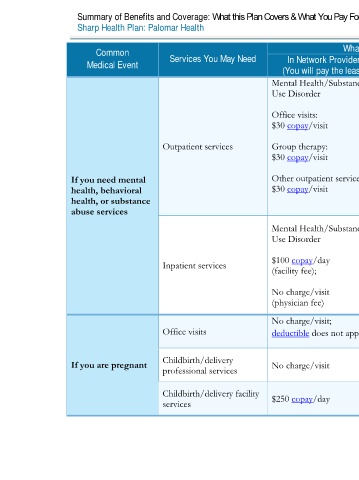
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2020 – 12/31/2020
Sharp Health Plan: Palomar Health Coverage for: Individual / Family | Plan Type: HDHP HMO
Common Services You May Need What You Will Pay Limitations, Exceptions, & Other Important
Medical Event In Network Provider Out-of-Network Provider Information
(You will pay the least) (You will pay the most)
Mental Health/Substance Mental Health/Substance
Use Disorder Use Disorder
Office visits: Office visits:
$30 copay/visit Not covered
Preauthorization is required. *Applies to
Outpatient services Group therapy: Group therapy: intensive outpatient program and partial
$30 copay/visit Not covered hospitalization program.
If you need mental Other outpatient services*: Other outpatient services*:
health, behavioral $30 copay/visit Not covered
health, or substance
abuse services
Mental Health/Substance Mental Health/Substance
Use Disorder Use Disorder
Preauthorization is required for non-
$100 copay/day $100 copay/day
Inpatient services emergency services. Out-of-network services
(facility fee); (facility fee); are covered for emergency care only.
No charge/visit No charge/visit
(physician fee) (physician fee)
No charge/visit;
Office visits deductible does not apply Not covered Cost sharing does not apply to certain
preventive services. Depending on the type of
services, a copayment, coinsurance, or
If you are pregnant Childbirth/delivery No charge/visit No charge/visit deductible (if applicable) may apply.
professional services Maternity care may include tests and services
described elsewhere in the SBC (i.e.
Childbirth/delivery facility $250 copay/day $250 copay/day ultrasound). Out-of-network services are
services covered for emergency care only.
4 of 11
Palomar Health HMO NG 2 L / ACCH15_40 / VSA8