
Page 29 - DIDC SOPS and Guidelinesv as of April 2019
P. 29
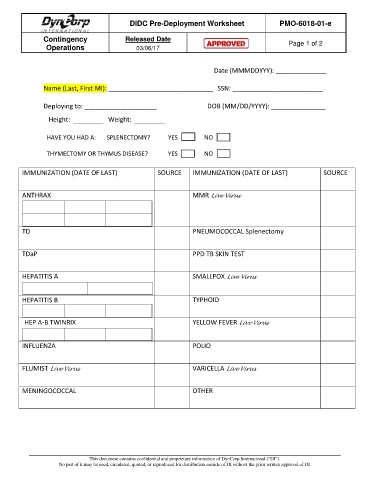
DIDC Pre-Deployment Worksheet PMO-6018-01-e
Contingency Released Date
Operations 03/06/17 Page 1 of 2
Date (MMMDDYYY): ______________
Name (Last, First MI): _____________________________ SSN: _________________________
Deploying to: ____________________ DOB (MM/DD/YYYY): _______________
Height: Weight:
HAVE YOU HAD A: SPLENECTOMY? YES NO
THYMECTOMY OR THYMUS DISEASE? YES NO
IMMUNIZATION (DATE OF LAST) SOURCE IMMUNIZATION (DATE OF LAST) SOURCE
ANTHRAX MMR Live Virus
TD PNEUMOCOCCAL Splenectomy
TDaP PPD TB SKIN TEST
HEPATITIS A SMALLPOX Live Virus
HEPATITIS B TYPHOID
HEP A-B TWINRIX YELLOW FEVER Live Virus
INFLUENZA POLIO
FLUMIST Live Virus VARICELLA Live Virus
MENINGOCOCCAL OTHER
This document contains confidential and proprietary information of DynCorp International (“DI”).
No part of it may be used, circulated, quoted, or reproduced for distribution outside of DI without the prior written approval of DI.