
Page 31 - DIDC SOPS and Guidelinesv as of April 2019
P. 31
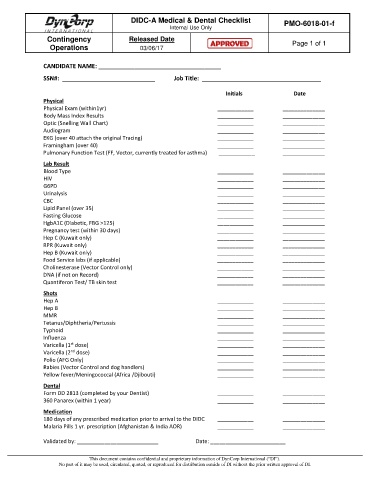
DIDC-A Medical & Dental Checklist PMO-6018-01-f
Internal Use Only
Contingency Released Date
Operations 03/06/17 Page 1 of 1
CANDIDATE NAME: _____________________________________
SSN#: ____________________________ Job Title: ____________________________________
Initials Date
Physical
Physical Exam (within1yr) ____________ ______________
Body Mass Index Results ____________ ______________
Optic (Snelling Wall Chart) ____________ ______________
Audiogram ____________ ______________
EKG (over 40 attach the original Tracing) ____________ ______________
Framingham (over 40) ____________ ______________
Pulmonary Function Test (FF, Vector, currently treated for asthma) ____________ ______________
Lab Result
Blood Type ____________ ______________
HIV ____________ ______________
G6PD ____________ ______________
Urinalysis ____________ ______________
CBC ____________ ______________
Lipid Panel (over 35) ____________ ______________
Fasting Glucose ____________ ______________
HgbA1C (Diabetic, FBG >125) ____________ ______________
Pregnancy test (within 30 days) ____________ ______________
Hep C (Kuwait only) ____________ ______________
RPR (Kuwait only) ____________ ______________
Hep B (Kuwait only) ____________ ______________
Food Service labs (if applicable) ____________ ______________
Cholinesterase (Vector Control only) ____________ ______________
DNA (if not on Record) ____________ ______________
Quantiferon Test/ TB skin test ____________ ______________
Shots
Hep A ____________ ______________
Hep B ____________ ______________
MMR ____________ ______________
Tetanus/Diphtheria/Pertussis ____________ ______________
Typhoid ____________ ______________
Influenza ____________ ______________
Varicella (1 dose) ____________ ______________
st
Varicella (2 dose) ____________ ______________
nd
Polio (AFG Only) ____________ ______________
Rabies (Vector Control and dog handlers) ____________ ______________
Yellow fever/Meningococcal (Africa /Djibouti) ____________ ______________
Dental
Form DD 2813 (completed by your Dentist) ____________ ______________
360 Panarex (within 1 year) ____________ ______________
Medication
180 days of any prescribed medication prior to arrival to the DIDC ____________ ______________
Malaria Pills 1 yr. prescription (Afghanistan & India AOR) ____________ ______________
Validated by: ___________________________ Date: _________________________
This document contains confidential and proprietary information of DynCorp International (“DI”).
No part of it may be used, circulated, quoted, or reproduced for distribution outside of DI without the prior written approval of DI.