
Page 1063 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 1063
CHAPTER 59 Special Aspects of Perinatal & Pediatric Pharmacology 1049
term, can induce fetal hepatic enzymes responsible for the gluc- can result in significant and irreversible renal damage in the fetus
uronidation of bilirubin, and the incidence of jaundice is lower and are therefore contraindicated in pregnant women. Adverse
in newborns when mothers are given phenobarbital than when effects may also be delayed, as in the case of female fetuses exposed
phenobarbital is not used. Before phototherapy became the pre- to diethylstilbestrol, who may be at increased risk for adenocarci-
ferred mode of therapy for neonatal indirect hyperbilirubinemia, noma of the vagina after puberty.
phenobarbital was used for this indication. Administration of
phenobarbital to the mother was suggested recently as a means D. Teratogenic Drug Actions
of decreasing the risk of intracranial bleeding in preterm infants. A single intrauterine exposure to a drug can affect the fetal struc-
However, large randomized studies failed to confirm this effect. tures undergoing rapid development at the time of exposure.
Antiarrhythmic drugs have also been given to mothers for treat- Thalidomide is an example of a drug that may profoundly affect
ment of fetal cardiac arrhythmias. Although their efficacy has not the development of the limbs after only brief exposure. This expo-
yet been established by controlled studies, digoxin, flecainide, pro- sure, however, must be at a critical time in the development of the
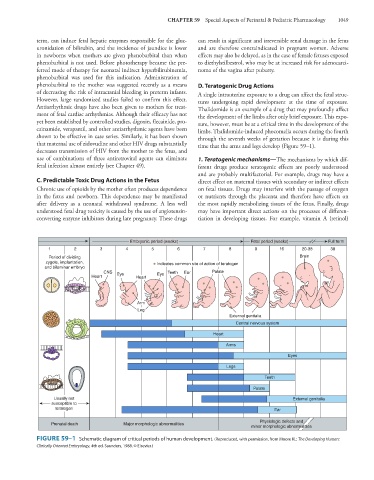
cainamide, verapamil, and other antiarrhythmic agents have been limbs. Thalidomide-induced phocomelia occurs during the fourth
shown to be effective in case series. Similarly, it has been shown through the seventh weeks of gestation because it is during this
that maternal use of zidovudine and other HIV drugs substantially time that the arms and legs develop (Figure 59–1).
decreases transmission of HIV from the mother to the fetus, and
use of combinations of three antiretroviral agents can eliminate 1. Teratogenic mechanisms—The mechanisms by which dif-
fetal infection almost entirely (see Chapter 49). ferent drugs produce teratogenic effects are poorly understood
and are probably multifactorial. For example, drugs may have a
C. Predictable Toxic Drug Actions in the Fetus direct effect on maternal tissues with secondary or indirect effects
Chronic use of opioids by the mother often produces dependence on fetal tissues. Drugs may interfere with the passage of oxygen
in the fetus and newborn. This dependence may be manifested or nutrients through the placenta and therefore have effects on
after delivery as a neonatal withdrawal syndrome. A less well the most rapidly metabolizing tissues of the fetus. Finally, drugs
understood fetal drug toxicity is caused by the use of angiotensin- may have important direct actions on the processes of differen-
converting enzyme inhibitors during late pregnancy. These drugs tiation in developing tissues. For example, vitamin A (retinol)
Embryonic period (weeks) Fetal period (weeks) Full term
1 2 3 4 5 6 7 8 9 16 20-38 38
Period of dividing Brain
zygote, implantation, Indicates common site of action of teratogen
and bilaminar embryo
CNS Eye Eye Teeth Ear Palate
Heart Heart
Arm
Leg
External genitalia
Central nervous system
Heart
Arms
Eyes
Legs
Teeth
Palate
Usually not External genitalia
susceptible to
teratogen Ear
Physiologic defects and
Prenatal death Major morphologic abnormalities
minor morphologic abnormalities
FIGURE 59–1 Schematic diagram of critical periods of human development. (Reproduced, with permission, from Moore KL: The Developing Human:
Clinically Oriented Embryology, 4th ed. Saunders, 1988. © Elsevier.)