
Page 1106 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 1106
1092 SECTION X Special Topics
OCH 3 OCH 3
CH 3 CH 3 OCH 3
N OCH 3 N OCF H
2
N CH 2 S N CH 2 S
O N O N
H H
Omeprazole Pantoprazole
O CH 2 CF 3
CH 3 H N N
CH S
N 2
CH 2 CH 2 N
N CH 2 S O
CH 3 O CH 2 O CH 3 Na
O N
Lansoprazole Rabeprazole
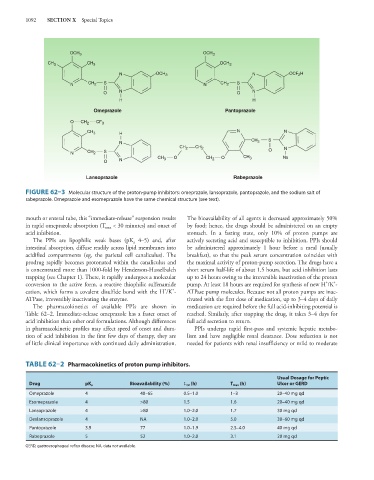
FIGURE 62–3 Molecular structure of the proton-pump inhibitors: omeprazole, lansoprazole, pantoprazole, and the sodium salt of
rabeprazole. Omeprazole and esomeprazole have the same chemical structure (see text).
mouth or enteral tube, this “immediate-release” suspension results The bioavailability of all agents is decreased approximately 50%
in rapid omeprazole absorption (T < 30 minutes) and onset of by food; hence, the drugs should be administered on an empty
max
acid inhibition. stomach. In a fasting state, only 10% of proton pumps are
The PPIs are lipophilic weak bases (pK 4–5) and, after actively secreting acid and susceptible to inhibition. PPIs should
a
intestinal absorption, diffuse readily across lipid membranes into be administered approximately 1 hour before a meal (usually
acidified compartments (eg, the parietal cell canaliculus). The breakfast), so that the peak serum concentration coincides with
prodrug rapidly becomes protonated within the canaliculus and the maximal activity of proton-pump secretion. The drugs have a
is concentrated more than 1000-fold by Henderson-Hasselbalch short serum half-life of about 1.5 hours, but acid inhibition lasts
trapping (see Chapter 1). There, it rapidly undergoes a molecular up to 24 hours owing to the irreversible inactivation of the proton
+
+
conversion to the active form, a reactive thiophilic sulfenamide pump. At least 18 hours are required for synthesis of new H /K -
+
+
cation, which forms a covalent disulfide bond with the H /K - ATPase pump molecules. Because not all proton pumps are inac-
ATPase, irreversibly inactivating the enzyme. tivated with the first dose of medication, up to 3–4 days of daily
The pharmacokinetics of available PPIs are shown in medication are required before the full acid-inhibiting potential is
Table 62–2. Immediate-release omeprazole has a faster onset of reached. Similarly, after stopping the drug, it takes 3–4 days for
acid inhibition than other oral formulations. Although differences full acid secretion to return.
in pharmacokinetic profiles may affect speed of onset and dura- PPIs undergo rapid first-pass and systemic hepatic metabo-
tion of acid inhibition in the first few days of therapy, they are lism and have negligible renal clearance. Dose reduction is not
of little clinical importance with continued daily administration. needed for patients with renal insufficiency or mild to moderate
TABLE 62–2 Pharmacokinetics of proton pump inhibitors.
Usual Dosage for Peptic
Drug pK a Bioavailability (%) t 1/2 (h) T max (h) Ulcer or GERD
Omeprazole 4 40–65 0.5–1.0 1–3 20–40 mg qd
Esomeprazole 4 >80 1.5 1.6 20–40 mg qd
Lansoprazole 4 >80 1.0–2.0 1.7 30 mg qd
Dexlansoprazole 4 NA 1.0–2.0 5.0 30–60 mg qd
Pantoprazole 3.9 77 1.0–1.9 2.5–4.0 40 mg qd
Rabeprazole 5 52 1.0–2.0 3.1 20 mg qd
GERD, gastroesophageal reflux disease; NA, data not available.