
Page 317 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 317
CHAPTER 17 Vasoactive Peptides 303
converting enzyme (Figure 17–1). ANG I may also be acted on by converted to ANG 1-7 by ACE. ACE2 also converts ANG II to ANG
1
plasma or tissue aminopeptidases to form [des-Asp ]angiotensin I; 1-7. ANG 1-7 has vasodilator activity, apparently mediated by the
1
this in turn is converted to [des-Asp ]angiotensin II (commonly orphan heterotrimeric guanine nucleotide-binding protein-coupled
known as angiotensin III) by converting enzyme. receptor (Mas receptor). This vasodilation may serve to counteract the
vasoconstrictor activity of ANG II. ACE2 also differs from ACE in
Converting Enzyme (Angiotensin- that it does not hydrolyze bradykinin and is not inhibited by convert-
Converting Enzyme [ACE], Peptidyl ing enzyme inhibitors (see below).
Dipeptidase, Kininase II) Angiotensinase
Converting enzyme is a dipeptidyl carboxypeptidase with two ANG II, which has a plasma half-life of 15–60 seconds, is
active sites that catalyzes the cleavage of dipeptides from the removed from the circulation by a variety of peptidases collectively
carboxyl terminal of certain peptides. Its most important substrates referred to as angiotensinase. It is metabolized during passage
are ANG I, which it converts to ANG II, and bradykinin, which through most vascular beds (a notable exception being the lung).
it inactivates (see Kinins, below). It also cleaves enkephalins and Most metabolites of ANG II are biologically inactive, but the ini-
substance P, but the physiologic significance of these effects has not tial product of aminopeptidase action—[des-Asp ]angiotensin II
1
been established. The action of converting enzyme is prevented by or angiotensin III—retains some biologic activity.
a penultimate prolyl residue in the substrate, and ANG II is there-
fore not hydrolyzed by converting enzyme. Converting enzyme is
distributed widely in the body. In most organs, converting enzyme ACTIONS OF ANGIOTENSIN II
is located on the luminal surface of vascular endothelial cells and is
thus in close contact with the circulation. ANG II exerts important actions at vascular smooth muscle,
A homolog of converting enzyme known as ACE2 is highly adrenal cortex, kidney, heart, and brain via the receptors described
expressed in vascular endothelial cells of the kidneys, heart, and below. Through these actions, the renin-angiotensin system plays
testes. Unlike converting enzyme, ACE2 has only one active site a key role in the regulation of fluid and electrolyte balance and
and functions as a carboxypeptidase rather than a dipeptidyl arterial blood pressure. Excessive activity of the renin-angiotensin
carboxypeptidase. It removes a single amino acid from the C-terminal system can result in hypertension and disorders of fluid and
of ANG I forming ANG 1-9 (Figure 17–3), which is inactive but is electrolyte homeostasis.
Blood Pressure
Angiotensinogen
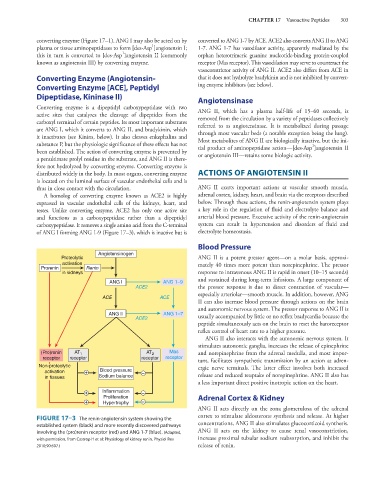
Proteolytic ANG II is a potent pressor agent—on a molar basis, approxi-
activation mately 40 times more potent than norepinephrine. The pressor
Prorenin Renin
in kidneys response to intravenous ANG II is rapid in onset (10–15 seconds)
and sustained during long-term infusions. A large component of
ANG I ANG 1–9
ACE2 the pressor response is due to direct contraction of vascular—
especially arteriolar—smooth muscle. In addition, however, ANG
ACE ACE
II can also increase blood pressure through actions on the brain
and autonomic nervous system. The pressor response to ANG II is
ANG II ANG 1–7 usually accompanied by little or no reflex bradycardia because the
ACE2
peptide simultaneously acts on the brain to reset the baroreceptor
reflex control of heart rate to a higher pressure.
ANG II also interacts with the autonomic nervous system. It
stimulates autonomic ganglia, increases the release of epinephrine
(Pro)renin AT 1 AT 2 Mas and norepinephrine from the adrenal medulla, and most impor-
receptor receptor receptor receptor tant, facilitates sympathetic transmission by an action at adren-
Non-proteolytic ergic nerve terminals. The latter effect involves both increased
activation + Blood pressure – release and reduced reuptake of norepinephrine. ANG II also has
in tissues Sodium balance
a less important direct positive inotropic action on the heart.
+ Inflammation –
Proliferation Adrenal Cortex & Kidney
+ Hypertrophy –
ANG II acts directly on the zona glomerulosa of the adrenal
cortex to stimulate aldosterone synthesis and release. At higher
FIGURE 17–3 The renin-angiotensin system showing the
established system (black) and more recently discovered pathways concentrations, ANG II also stimulates glucocorticoid synthesis.
involving the (pro)renin receptor (red) and ANG 1-7 (blue). (Adapted, ANG II acts on the kidney to cause renal vasoconstriction,
with permission, from Castrop H et al: Physiology of kidney renin. Physiol Rev increase proximal tubular sodium reabsorption, and inhibit the
2010;90:607.) release of renin.