
Page 508 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 508
494 SECTION V Drugs That Act in the Central Nervous System
Dopamine receptors are discussed in detail in Chapters 21 and
Normal 29. They exist in five subtypes. D and D receptors are classified
5
1
Substantia Corpus as the D receptor family based on genetic and biochemical fac-
1
nigra striatum tors; D , D , and D are grouped as belonging to the D receptor
4
2
3
2
family. Dopamine receptors of the D type are located in the pars
1
Dopamine compacta of the substantia nigra and presynaptically on striatal
axons coming from cortical neurons and from dopaminergic
Acetyl- GABA cells in the substantia nigra. The D receptors are located post-
2
choline
synaptically on striatal neurons and presynaptically on axons in
the substantia nigra belonging to neurons in the basal ganglia.
Parkinsonism The benefits of dopaminergic antiparkinsonism drugs appear
to depend mostly on stimulation of the D receptors. However,
2
D -receptor stimulation may also be required for maximal benefit,
1
and one of the newer drugs is D selective. Dopamine agonist or
3
partial agonist ergot derivatives such as lergotrile and bromocrip-
tine that are powerful stimulators of the D receptors have anti-
2
parkinsonism properties, whereas certain dopamine blockers that
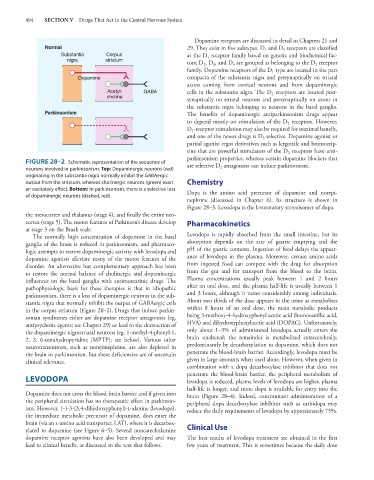
FIGURE 28–2 Schematic representation of the sequence of are selective D antagonists can induce parkinsonism.
neurons involved in parkinsonism. Top: Dopaminergic neurons (red) 2
originating in the substantia nigra normally inhibit the GABAergic
output from the striatum, whereas cholinergic neurons (green) exert Chemistry
an excitatory effect. Bottom: In parkinsonism, there is a selective loss Dopa is the amino acid precursor of dopamine and norepi-
of dopaminergic neurons (dashed, red).
nephrine (discussed in Chapter 6). Its structure is shown in
Figure 28–3. Levodopa is the levorotatory stereoisomer of dopa.
the mesocortex and thalamus (stage 4), and finally the entire neo-
cortex (stage 5). The motor features of Parkinson’s disease develop Pharmacokinetics
at stage 3 on the Braak scale.
The normally high concentration of dopamine in the basal Levodopa is rapidly absorbed from the small intestine, but its
ganglia of the brain is reduced in parkinsonism, and pharmaco- absorption depends on the rate of gastric emptying and the
logic attempts to restore dopaminergic activity with levodopa and pH of the gastric contents. Ingestion of food delays the appear-
dopamine agonists alleviate many of the motor features of the ance of levodopa in the plasma. Moreover, certain amino acids
disorder. An alternative but complementary approach has been from ingested food can compete with the drug for absorption
to restore the normal balance of cholinergic and dopaminergic from the gut and for transport from the blood to the brain.
influences on the basal ganglia with antimuscarinic drugs. The Plasma concentrations usually peak between 1 and 2 hours
pathophysiologic basis for these therapies is that in idiopathic after an oral dose, and the plasma half-life is usually between 1
parkinsonism, there is a loss of dopaminergic neurons in the sub- and 3 hours, although it varies considerably among individuals.
stantia nigra that normally inhibit the output of GABAergic cells About two thirds of the dose appears in the urine as metabolites
in the corpus striatum (Figure 28–2). Drugs that induce parkin- within 8 hours of an oral dose, the main metabolic products
sonian syndromes either are dopamine receptor antagonists (eg, being 3-methoxy-4-hydroxyphenyl acetic acid (homovanillic acid,
antipsychotic agents; see Chapter 29) or lead to the destruction of HVA) and dihydroxyphenylacetic acid (DOPAC). Unfortunately,
the dopaminergic nigrostriatal neurons (eg, 1-methyl-4-phenyl-1, only about 1–3% of administered levodopa actually enters the
2, 3, 6-tetrahydropyridine [MPTP]; see below). Various other brain unaltered; the remainder is metabolized extracerebrally,
neurotransmitters, such as norepinephrine, are also depleted in predominantly by decarboxylation to dopamine, which does not
the brain in parkinsonism, but these deficiencies are of uncertain penetrate the blood-brain barrier. Accordingly, levodopa must be
clinical relevance. given in large amounts when used alone. However, when given in
combination with a dopa decarboxylase inhibitor that does not
penetrate the blood-brain barrier, the peripheral metabolism of
LEVODOPA levodopa is reduced, plasma levels of levodopa are higher, plasma
half-life is longer, and more dopa is available for entry into the
Dopamine does not cross the blood-brain barrier and if given into brain (Figure 28–4). Indeed, concomitant administration of a
the peripheral circulation has no therapeutic effect in parkinson- peripheral dopa decarboxylase inhibitor such as carbidopa may
ism. However, (–)-3-(3,4-dihydroxyphenyl)-l-alanine (levodopa), reduce the daily requirements of levodopa by approximately 75%.
the immediate metabolic precursor of dopamine, does enter the
brain (via an l-amino acid transporter, LAT), where it is decarbox- Clinical Use
ylated to dopamine (see Figure 6–5). Several noncatecholamine
dopamine receptor agonists have also been developed and may The best results of levodopa treatment are obtained in the first
lead to clinical benefit, as discussed in the text that follows. few years of treatment. This is sometimes because the daily dose