
Page 869 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 869
CHAPTER 48 Antifungal Agents 855
Fungal cell Fungal cell membrane and cell wall
Proteins
β-glucans
Chitin
DNA, RNA
synthesis
Cell membrane
–
bilayer
Flucytosine
β-glucan
Squalene Ergosterol Amphotericin B, synthase
nystatin
– Terbinafine –
– Azoles Echinocandins
Squalene epoxide Lanosterol
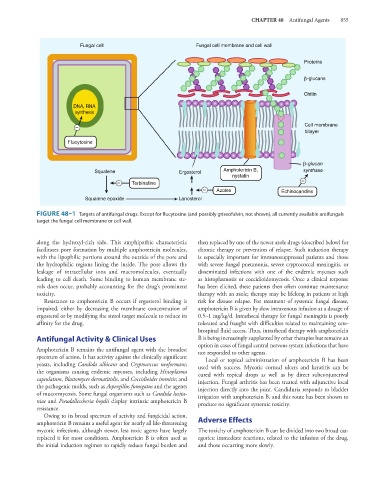
FIGURE 48–1 Targets of antifungal drugs. Except for flucytosine (and possibly griseofulvin, not shown), all currently available antifungals
target the fungal cell membrane or cell wall.
along the hydroxyl-rich side. This amphipathic characteristic then replaced by one of the newer azole drugs (described below) for
facilitates pore formation by multiple amphotericin molecules, chronic therapy or prevention of relapse. Such induction therapy
with the lipophilic portions around the outside of the pore and is especially important for immunosuppressed patients and those
the hydrophilic regions lining the inside. The pore allows the with severe fungal pneumonia, severe cryptococcal meningitis, or
leakage of intracellular ions and macromolecules, eventually disseminated infections with one of the endemic mycoses such
leading to cell death. Some binding to human membrane ste- as histoplasmosis or coccidioidomycosis. Once a clinical response
rols does occur, probably accounting for the drug’s prominent has been elicited, these patients then often continue maintenance
toxicity. therapy with an azole; therapy may be lifelong in patients at high
Resistance to amphotericin B occurs if ergosterol binding is risk for disease relapse. For treatment of systemic fungal disease,
impaired, either by decreasing the membrane concentration of amphotericin B is given by slow intravenous infusion at a dosage of
ergosterol or by modifying the sterol target molecule to reduce its 0.5–1 mg/kg/d. Intrathecal therapy for fungal meningitis is poorly
affinity for the drug. tolerated and fraught with difficulties related to maintaining cere-
brospinal fluid access. Thus, intrathecal therapy with amphotericin
Antifungal Activity & Clinical Uses B is being increasingly supplanted by other therapies but remains an
option in cases of fungal central nervous system infections that have
Amphotericin B remains the antifungal agent with the broadest not responded to other agents.
spectrum of action. It has activity against the clinically significant Local or topical administration of amphotericin B has been
yeasts, including Candida albicans and Cryptococcus neoformans; used with success. Mycotic corneal ulcers and keratitis can be
the organisms causing endemic mycoses, including Histoplasma cured with topical drops as well as by direct subconjunctival
capsulatum, Blastomyces dermatitidis, and Coccidioides immitis; and injection. Fungal arthritis has been treated with adjunctive local
the pathogenic molds, such as Aspergillus fumigatus and the agents injection directly into the joint. Candiduria responds to bladder
of mucormycosis. Some fungal organisms such as Candida lusita- irrigation with amphotericin B, and this route has been shown to
niae and Pseudallescheria boydii display intrinsic amphotericin B produce no significant systemic toxicity.
resistance.
Owing to its broad spectrum of activity and fungicidal action,
amphotericin B remains a useful agent for nearly all life-threatening Adverse Effects
mycotic infections, although newer, less toxic agents have largely The toxicity of amphotericin B can be divided into two broad cat-
replaced it for most conditions. Amphotericin B is often used as egories: immediate reactions, related to the infusion of the drug,
the initial induction regimen to rapidly reduce fungal burden and and those occurring more slowly.