
Page 40 - SAMPLE
P. 40
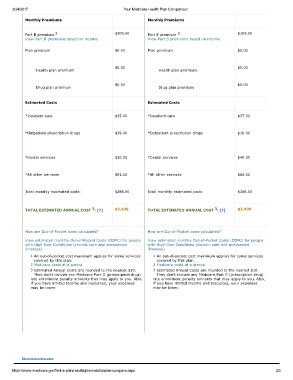
2/24/2017 Your Medicare Health Plan Comparison
Monthly Premiums Monthly Premiums
2
2
Part B premium $109.00 Part B premium $109.00
View Part B premiums based on income View Part B premiums based on income
Plan premium $0.00 Plan premium $0.00
$0.00 $0.00
Health plan premium Health plan premium
$0.00 $0.00
Drug plan premium Drug plan premium
Estimated Costs Estimated Costs
*Inpatient care $35.00 *Inpatient care $37.00
*Outpatient prescription drugs $39.00 *Outpatient prescription drugs $16.00
*Dental services $10.00 *Dental services $40.00
*All other services $93.00 *All other services $84.00
Total monthly estimated costs: $286.00 Total monthly estimated costs: $286.00
3
3
TOTAL ESTIMATED ANNUAL COST : [?] $3,430 TOTAL ESTIMATED ANNUAL COST : [?] $3,430
How are OutofPocket costs calculated? How are OutofPocket costs calculated?
View estimated monthly OutofPocket Costs (OOPC) for people View estimated monthly OutofPocket Costs (OOPC) for people
with HighCost Conditions (chronic care and unexpected with HighCost Conditions (chronic care and unexpected
illnesses) illnesses)
1 An outofpocket cost maximum applies for some services 1 An outofpocket cost maximum applies for some services
covered by this plan. covered by this plan.
2 Medicare costs at a glance 2 Medicare costs at a glance
3 Estimated Annual Costs are rounded to the nearest $10. 3 Estimated Annual Costs are rounded to the nearest $10.
They don't include any Medicare Part D (prescription drug) They don't include any Medicare Part D (prescription drug)
late enrollment penalty amounts that may apply to you. Also, late enrollment penalty amounts that may apply to you. Also,
if you have limited income and resources, your expenses if you have limited income and resources, your expenses
may be lower. may be lower.
Return to previous page
https://www.medicare.gov/findaplan/results/planresults/plancompare.aspx 3/3