
Page 42 - SAMPLE
P. 42
2/24/2017 Your Medicare Health Plan Comparison
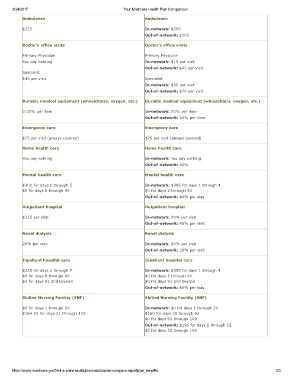
Ambulance Ambulance
$225 Innetwork: $205
Outofnetwork: $205
Doctor's office visits Doctor's office visits
Primary Physician Primary Physician
You pay nothing Innetwork: $15 per visit
Outofnetwork: $45 per visit
Specialist
$45 per visit Specialist
Innetwork: $50 per visit
Outofnetwork: $70 per visit
Durable medical equipment (wheelchairs, oxygen, etc.) Durable medical equipment (wheelchairs, oxygen, etc.)
020% per item Innetwork: 20% per item
Outofnetwork: 50% per item
Emergency care Emergency care
$75 per visit (always covered) $75 per visit (always covered)
Home health care Home health care
You pay nothing Innetwork: You pay nothing
Outofnetwork: 50%
Mental health care Mental health care
$300 for days 1 through 5 Innetwork: $395 for days 1 through 4
$0 for days 6 through 90 $0 for days 5 through 90
Outofnetwork: 40% per stay
Outpatient hospital Outpatient hospital
$325 per visit Innetwork: 20% per visit
Outofnetwork: 40% per visit
Renal dialysis Renal dialysis
20% per visit Innetwork: 20% per visit
Outofnetwork: 20% per visit
Inpatient hospital care Inpatient hospital care
$225 for days 1 through 7 Innetwork: $395 for days 1 through 4
$0 for days 8 through 90 $0 for days 5 through 90
$0 for days 91 and beyond $0 for days 91 and beyond
Outofnetwork: 40% per stay
Skilled Nursing Facility (SNF) Skilled Nursing Facility (SNF)
$0 for days 1 through 20 Innetwork: $0 for days 1 through 20
$164.50 for days 21 through 100 $160 for days 21 through 62
$0 for days 63 through 100
Outofnetwork: $195 for days 1 through 52
$0 for days 53 through 100
https://www.medicare.gov/findaplan/results/planresults/plancompare.aspx#plan_benefits 2/3