
Page 12 - Cover Letter and Medicare Evaluation for Jamie Marshall
P. 12
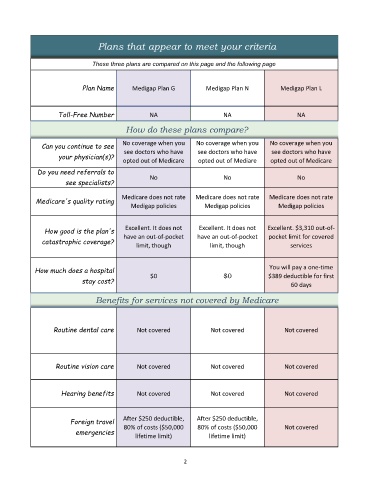
Plans that appear to meet your criteria
These three plans are compared on this page and the following page
Plan Name Medigap Plan G Medigap Plan N Medigap Plan L
Toll-Free Number NA NA NA
QuaSection Heading How do these plans compare?
lity ratings from
Can you continue to see No coverage when you No coverage when you No coverage when you
your physician(s)? see doctors who have see doctors who have see doctors who have
opted out of Medicare opted out of Mediare opted out of Medicare
Do you need referrals to
see specialists? No No No
Medicare does not rate Medicare does not rate Medicare does not rate
Medicare's quality rating
Medigap policies Medigap policies Medigap policies
How good is the plan's Excellent. It does not Excellent. It does not Excellent. $3,310 out-of-
catastrophic coverage? have an out-of-pocket have an out-of-pocket pocket limit for covered
limit, though limit, though services
How much does a hospital You will pay a one-time
stay cost? $0 $0 $389 deductible for first
60 days
Benefits for services not covered by Medicare
Routine dental care Not covered Not covered Not covered
Routine vision care Not covered Not covered Not covered
Hearing benefits Not covered Not covered Not covered
Foreign travel After $250 deductible, After $250 deductible,
emergencies 80% of costs ($50,000 80% of costs ($50,000 Not covered
lifetime limit)
lifetime limit)
2