
Page 91 - Evaluation for Tom Tappan
P. 91
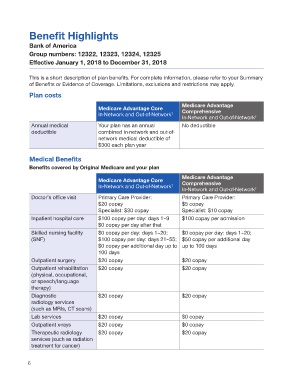
Benefit Highlights
Bank of America
Group numbers: 12322, 12323, 12324, 12325
Effective January 1, 2018 to December 31, 2018
This is a short description of plan benefits. For complete information, please refer to your Summary
of Benefits or Evidence of Coverage. Limitations, exclusions and restrictions may apply.
Plan costs
Medicare Advantage
Medicare Advantage Core
In-Network and Out-of-Network † Comprehensive
In-Network and Out-of-Network †
Annual medical Your plan has an annual No deductible
deductible combined in-network and out-of-
network medical deductible of
$300 each plan year
Medical Benefits
Benefits covered by Original Medicare and your plan
Medicare Advantage
Medicare Advantage Core Comprehensive
In-Network and Out-of-Network †
In-Network and Out-of-Network †
Doctor’s office visit Primary Care Provider: Primary Care Provider:
$20 copay $5 copay
Specialist: $30 copay Specialist: $10 copay
Inpatient hospital care $100 copay per day: days 1–9 $100 copay per admission
$0 copay per day after that
Skilled nursing facility $0 copay per day: days 1–20; $0 copay per day: days 1–20;
(SNF) $100 copay per day: days 21–55; $50 copay per additional day
$0 copay per additional day up to up to 100 days
100 days
Outpatient surgery $20 copay $20 copay
Outpatient rehabilitation $20 copay $20 copay
(physical, occupational,
or speech/language
therapy)
Diagnostic $20 copay $20 copay
radiology services
(such as MRIs, CT scans)
Lab services $20 copay $0 copay
Outpatient x-rays $20 copay $0 copay
Therapeutic radiology $20 copay $20 copay
services (such as radiation
treatment for cancer)