
Page 32 - Cover Letter and Evaluation for Chris Parlin
P. 32
10/10/2017 Your Plan Results
Your Plan Results
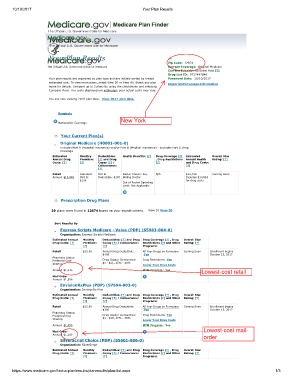
Zip Code: 12874
Current Coverage: Original Medicare
Current Subsidy: No Extra Help [?]
Drug List ID: 9757447840
Your plan results are organized by plan type and are initially sorted by lowest Password Date: 10/10/2017
estimated cost. To view more plans, select View 20 or View All. Select any plan Important Coverage Information
name for details. Compare up to 3 plans by using the checkboxes and selecting
Compare Plans. The costs displayed are estimates; your actual costs may vary.
You are now viewing 2018 plan data. View 2017 plan data.
Symbols
New York
Nationwide Coverage
Your Current Plan(s)
Original Medicare (H0001-001-0)
Includes Part A (Hospital Insurance) and/or Part B (Medical Insurance) - Excludes Part D Drug
Coverage
Estimated Monthly Deductibles: Health Benefits: [?] Drug Coverage [?] Estimated Overall Star
Annual Drug Premium: [?] and Drug , Drug Restrictions Annual Health Rating: [?]
Costs: [?] [?] Copay [?] / [?] and Drug Costs:
Coinsurance: [?]
[?]
Retail Standard Part B Doctor Choice: Any N/A $14,740 Coming Soon
Annual: $10,863 Part B: Deductible: $183 Willing Doctor Includes $10,863
$134 for drug costs
Out of Pocket Spending
Limit: Not Applicable
Prescription Drug Plans
20 plans were found in 12874 based on your search criteria. View 10 View 20
Sort Results By
Express Scripts Medicare - Value (PDP) (S5983-004-0)
Organization: Express Scripts Medicare
Estimated Annual Monthly Deductibles: [?] and Drug Drug Coverage [?] , Drug Overall Star
Drug Costs: [?] Premium: Copay [?] / Coinsurance: Restrictions [?] and Other Rating: [?]
[?] [?] Programs:
Retail $35.00 Annual Drug Deductible: All Your Drugs on Formulary Coming Soon Enrollment begins
$405 :Yes October 15, 2017
Pharmacy Status:
Preferred Cost- Drug Copay/ Coinsurance: Drug Restrictions: Yes
Sharing $1 - $21, 25% - 48% Lower Your Drug Costs
Annual: $1,435 MTM Program : Yes
Lowest-cost retail
Mail Order
Annual: $1,586
EnvisionRxPlus (PDP) (S7694-003-0)
Organization: EnvisionRx Plus
Estimated Annual Monthly Deductibles: [?] and Drug Drug Coverage [?] , Drug Overall Star
Drug Costs: [?] Premium: Copay [?] / Coinsurance: Restrictions [?] and Other Rating: [?]
[?] [?] Programs:
Retail $12.60 Annual Drug Deductible: All Your Drugs on Formulary Coming Soon Enrollment begins
$300 :Yes October 15, 2017
Pharmacy Status:
Preferred Cost- Drug Copay/ Coinsurance: Drug Restrictions: Yes
Sharing $1 - $29, 27% - 38% Lower Your Drug Costs
Annual: $1,455 MTM Program : Yes
Mail Order Lowest-cost mail-
Annual: $1,285 order
SilverScript Choice (PDP) (S5601-006-0)
Organization: SilverScript
Estimated Annual Monthly Deductibles: [?] and Drug Drug Coverage [?] , Drug Overall Star
Drug Costs: [?] Premium: Copay [?] / Coinsurance: Restrictions [?] and Other Rating: [?]
[?] [?] Programs:
https://www.medicare.gov/find-a-plan/results/planresults/plan-list.aspx 1/3