
Page 57 - Cover Letter and Evaluation for Mike Peaseley
P. 57
11/17/2017 Your Plan Results
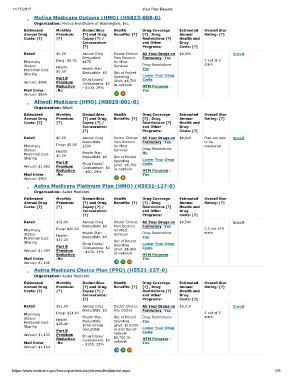
Molina Medicare Options (HMO) (H5823-008-0)
Organization: Molina Healthcare of Washington, Inc.
Estimated Monthly Deductibles Health Drug Coverage Estimated Overall Star
Annual Drug Premium: [?] and Drug Benefits: [?] [?] , Drug Annual Rating: [?]
Costs: [?] [?] Copay [?] / Restrictions [?] Health and
Coinsurance: and Other Drug
[?] Programs: Costs: [?]
Retail $0.00 Annual Drug Doctor Choice: All Your Drugs on $4,650 Enroll
Deductible: Plan Doctors Formulary :Yes
Pharmacy Drug: $0.00 $175 for Most 3 out of 5
Status: Health: Services Drug Restrictions: stars
Preferred Cost- $0.00 Health Plan Yes
Sharing Deductible: $0 Out of Pocket Lower Your Drug
Part B Drug Copay/ Spending Costs
Annual: $986 Premium Coinsurance: $2 Limit: $6,700
Reduction - $100, 29% In-network MTM Program :
Mail Order :No Yes
Annual: $864
Allwell Medicare (HMO) (H0029-001-0)
Organization: Allwell
Estimated Monthly Deductibles Health Drug Coverage Estimated Overall Star
Annual Drug Premium: [?] and Drug Benefits: [?] [?] , Drug Annual Rating: [?]
Costs: [?] [?] Copay [?] / Restrictions [?] Health and
Coinsurance: and Other Drug
[?] Programs: Costs: [?]
Retail $0.00 Annual Drug Doctor Choice: All Your Drugs on $4,840 Plan too new Enroll
Deductible: Plan Doctors Formulary :Yes to be
Pharmacy Drug: $0.00 $200 for Most measured
Status: Health: Services Drug Restrictions:
Preferred Cost- $0.00 Health Plan No
Sharing Deductible: $0 Out of Pocket Lower Your Drug
Part B Drug Copay/ Spending Costs
Annual: $1,062 Premium Coinsurance: $0 Limit: $6,700
Reduction - $90, 29% In-network MTM Program :
Mail Order :No Yes
Annual: $983
Aetna Medicare Platinum Plan (HMO) (H3931-127-0)
Organization: Aetna Medicare
Estimated Monthly Deductibles Health Drug Coverage Estimated Overall Star
Annual Drug Premium: [?] and Drug Benefits: [?] [?] , Drug Annual Rating: [?]
Costs: [?] [?] Copay [?] / Restrictions [?] Health and
Coinsurance: and Other Drug
[?] Programs: Costs: [?]
Retail $32.00 Annual Drug Doctor Choice: All Your Drugs on $4,590 Enroll
Deductible: $0 Plan Doctors Formulary :Yes
Pharmacy Drug: $20.80 for Most 3.5 out of 5
Status: Health: Health Plan Services Drug Restrictions: stars
Preferred Cost- $11.20 Deductible: $0 Yes
Sharing Drug Copay/ Out of Pocket Lower Your Drug
Part B Coinsurance: $0 Spending Costs
Annual: $1,084 Premium - $100, 33% Limit: $5,900
Reduction In-network MTM Program :
Mail Order :No Yes
Annual: $1,106
Aetna Medicare Choice Plan (PPO) (H5521-127-0)
Organization: Aetna Medicare
Estimated Monthly Deductibles Health Drug Coverage Estimated Overall Star
Annual Drug Premium: [?] and Drug Benefits: [?] [?] , Drug Annual Rating: [?]
Costs: [?] [?] Copay [?] / Restrictions [?] Health and
Coinsurance: and Other Drug
[?] Programs: Costs: [?]
Retail $51.00 Annual Drug Doctor Choice: All Your Drugs on $5,010 Enroll
Deductible: $0 Any Doctor Formulary :Yes
Pharmacy Drug: $24.60 4 out of 5
Status: Health: Health Plan Out of Pocket Drug Restrictions: stars
Preferred Cost- $26.40 Deductible: Spending Yes
Sharing $750 annual Limit: $10,000 Lower Your Drug
Part B deductible In and Out-of- Costs
Annual: $1,130 Premium Drug Copay/ network
Reduction Coinsurance: $0 $6,700 In- MTM Program :
Mail Order :No - $100, 33% network Yes
Annual: $1,152
https://www.medicare.gov/find-a-plan/results/planresults/plan-list.aspx 2/6