
Page 60 - Cover Letter and Evaluation for Mike Peaseley
P. 60
11/17/2017 Your Plan Results
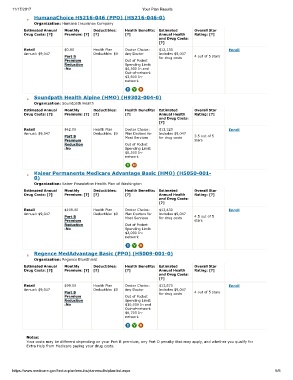
HumanaChoice H5216-046 (PPO) (H5216-046-0)
Organization: Humana Insurance Company
Estimated Annual Monthly Deductibles: Health Benefits: Estimated Overall Star
Drug Costs: [?] Premium: [?] [?] [?] Annual Health Rating: [?]
and Drug Costs:
[?]
Retail $0.00 Health Plan Doctor Choice: $12,130 Enroll
Annual: $9,047 Deductible: $0 Any Doctor Includes $9,047
Part B for drug costs 4 out of 5 stars
Premium Out of Pocket
Reduction Spending Limit:
:No $4,500 In and
Out-of-network
$3,600 In-
network
Soundpath Health Alpine (HMO) (H9302-004-0)
Organization: Soundpath Health
Estimated Annual Monthly Deductibles: Health Benefits: Estimated Overall Star
Drug Costs: [?] Premium: [?] [?] [?] Annual Health Rating: [?]
and Drug Costs:
[?]
Retail $42.00 Health Plan Doctor Choice: $13,320 Enroll
Annual: $9,047 Deductible: $0 Plan Doctors for Includes $9,047
Part B Most Services for drug costs 3.5 out of 5
Premium stars
Reduction Out of Pocket
:No Spending Limit:
$6,500 In-
network
Kaiser Permanente Medicare Advantage Basic (HMO) (H5050-001-
0)
Organization: Kaiser Foundation Health Plan of Washington
Estimated Annual Monthly Deductibles: Health Benefits: Estimated Overall Star
Drug Costs: [?] Premium: [?] [?] [?] Annual Health Rating: [?]
and Drug Costs:
[?]
Retail $109.00 Health Plan Doctor Choice: $13,430 Enroll
Annual: $9,047 Deductible: $0 Plan Doctors for Includes $9,047
Part B Most Services for drug costs 4.5 out of 5
Premium stars
Reduction Out of Pocket
:No Spending Limit:
$2,000 In-
network
Regence MedAdvantage Basic (PPO) (H5009-001-0)
Organization: Regence BlueShield
Estimated Annual Monthly Deductibles: Health Benefits: Estimated Overall Star
Drug Costs: [?] Premium: [?] [?] [?] Annual Health Rating: [?]
and Drug Costs:
[?]
Retail $99.00 Health Plan Doctor Choice: $13,670 Enroll
Annual: $9,047 Deductible: $0 Any Doctor Includes $9,047
Part B for drug costs 4 out of 5 stars
Premium Out of Pocket
Reduction Spending Limit:
:No $10,000 In and
Out-of-network
$6,700 In-
network
Notes:
Your costs may be different depending on your Part B premium, any Part D penalty that may apply, and whether you qualify for
Extra Help from Medicare paying your drug costs.
https://www.medicare.gov/find-a-plan/results/planresults/plan-list.aspx 5/6