
Page 94 - Cover Letter and Evaluation for Mike Peaseley
P. 94
11/17/2017 Your Medicare Health Plan Comparison
Return to previous page
Your Plan Comparison
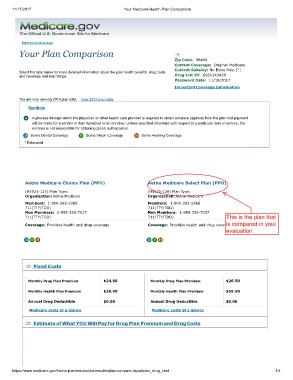
Zip Code: 98499
Current Coverage: Original Medicare
Current Subsidy: No Extra Help [?]
Select the tabs below for more detailed information about the plan health benefits, drug costs
and coverage and star ratings. Drug List ID: 6951340928
Password Date: 11/16/2017
Important Coverage Information
You are now viewing 2018 plan data. View 2017 plan data.
Symbols
A process through which the physician or other health care provider is required to obtain advance approval from the plan that payment
will be made for a service or item furnished to an enrollee. Unless specified otherwise with respect to a particular item or service, the
enrollee is not responsible for obtaining (prior) authorization.
Some Dental Coverage Some Vision Coverage Some Hearing Coverage
* Estimated
Aetna Medicare Choice Plan (PPO) Aetna Medicare Select Plan (PPO)
(H5521-127) Plan Type: (H5521-128) Plan Type:
Organization: Aetna Medicare Organization: Aetna Medicare
Members: 1-800-282-5366 Members: 1-800-282-5366
711(TTY/TDD) 711(TTY/TDD)
Non Members: 1-855-338-7027 Non Members: 1-855-338-7027
711(TTY/TDD) 711(TTY/TDD) This is the plan that
is
Coverage: Provides health and drug coverage Coverage: Provides health and drug coveragecompared in your
evaluation.
Fixed Costs
Monthly Drug Plan Premium $24.60 Monthly Drug Plan Premium $26.50
Monthly Health Plan Premium $26.40 Monthly Health Plan Premium $59.50
Annual Drug Deductible $0.00 Annual Drug Deductible $0.00
Medicare costs at a glance Medicare costs at a glance
Estimate of What YOU Will Pay for Drug Plan Premium and Drug Costs
https://www.medicare.gov/find-a-plan/results/planresults/plan-compare.aspx#plan_drug_cost 1/4