
Page 96 - Cover Letter and Evaluation for Mike Peaseley
P. 96
11/17/2017 Your Medicare Health Plan Comparison
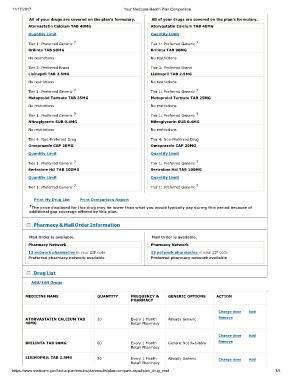
All of your drugs are covered on the plan’s formulary. All of your drugs are covered on the plan’s formulary.
Atorvastatin Calcium TAB 40MG Atorvastatin Calcium TAB 40MG
Quantity Limit Quantity Limit
Tier 1: Preferred Generic 7 Tier 1: Preferred Generic 7
Brilinta TAB 90MG Brilinta TAB 90MG
No restrictions No restrictions
Tier 3: Preferred Brand Tier 3: Preferred Brand
Lisinopril TAB 2.5MG Lisinopril TAB 2.5MG
No restrictions No restrictions
Tier 1: Preferred Generic 7 Tier 1: Preferred Generic 7
Metoprolol Tartrate TAB 25MG Metoprolol Tartrate TAB 25MG
No restrictions No restrictions
Tier 1: Preferred Generic 7 Tier 1: Preferred Generic 7
Nitroglycerin SUB 0.4MG Nitroglycerin SUB 0.4MG
No restrictions No restrictions
Tier 4: Non-Preferred Drug Tier 4: Non-Preferred Drug
Omeprazole CAP 20MG Omeprazole CAP 20MG
Quantity Limit Quantity Limit
Tier 1: Preferred Generic 7 Tier 1: Preferred Generic 7
Sertraline Hcl TAB 100MG Sertraline Hcl TAB 100MG
Quantity Limit Quantity Limit
Tier 1: Preferred Generic 7 Tier 1: Preferred Generic 7
Print My Drug List Print Comparison Report
7 The price displayed for this drug may be lower than what you would typically pay during this period because of
additional gap coverage offered by this plan.
Pharmacy & Mail Order Information
Mail Order is available. Mail Order is available.
Pharmacy Network Pharmacy Network
13 network pharmacies in your ZIP code 13 network pharmacies in your ZIP code
Preferred pharmacy network available Preferred pharmacy network available
Drug List
Add/Edit Drugs
MEDICINE NAME QUANTITY FREQUENCY & GENERIC OPTIONS ACTION
PHARMACY
Change dose Add
ATORVASTATIN CALCIUM TAB 30 Every 1 Month Already Generic Remove
40MG Retail Pharmacy
Change dose Add
BRILINTA TAB 90MG 60 Every 1 Month Generic Not Available Remove
Retail Pharmacy
LISINOPRIL TAB 2.5MG 30 Every 1 Month Already Generic Change dose Add
Retail Pharmacy
https://www.medicare.gov/find-a-plan/results/planresults/plan-compare.aspx#plan_drug_cost 3/4