Page 17 - Dentsu 2022 Annual Enrollment Flyer
P. 17
Vision Benefits
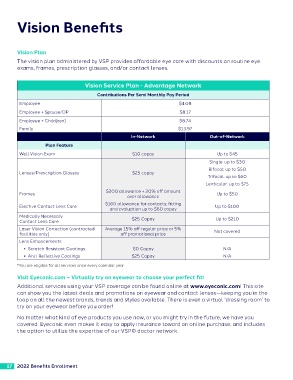
Vision Plan
The vision plan administered by VSP provides affordable eye care with discounts on routine eye
exams, frames, prescription glasses, and/or contact lenses.
Vision Service Plan - Advantage Network
Contributions Per Semi Monthly Pay Period
Employee $4.08
Employee + Spouse/DP $8.17
Employee + Child(ren) $8.74
Family $13.97
In-Network Out-of-Network
Plan Feature
Well Vision Exam $10 copay Up to $45
Single: up to $30
Bifocal: up to $50
Lenses/Prescription Glasses $25 copay
Trifocal: up to $60
Lenticular: up to $75
Frames $200 allowance + 20% off amount Up to $50
over allowance
Elective Contact Lens Care $160 allowance for contacts; fitting Up to $100
and evaluation up to $60 copay
Medically Necessary $25 Copay Up to $210
Contact Lens Care
Laser Vision Correction (contracted Average 15% off regular price or 5% Not covered
facilities only) off promotional price
Lens Enhancements
• Scratch Resistant Coatings $0 Copay N/A
• Anti-Reflective Coatings $25 Copay N/A
*You are eligible for all services once every calendar year
Visit Eyeconic.com – Virtually try on eyewear to choose your perfect fit!
Additional services using your VSP coverage can be found online at www.eyeconic.com! This site
can show you the latest deals and promotions on eyewear and contact lenses—keeping you in the
loop on all the newest brands, trends and styles available. There is even a virtual ‘dressing room’ to
try on your eyewear before you order!
No matter what kind of eye products you use now, or you might try in the future, we have you
covered. Eyeconic even makes it easy to apply insurance toward an online purchase, and includes
the option to utilize the expertise of our VSP© doctor network.
17 2022 Benefits Enrollment
Vision Plan
The vision plan administered by VSP provides affordable eye care with discounts on routine eye
exams, frames, prescription glasses, and/or contact lenses.
Vision Service Plan - Advantage Network
Contributions Per Semi Monthly Pay Period
Employee $4.08
Employee + Spouse/DP $8.17
Employee + Child(ren) $8.74
Family $13.97
In-Network Out-of-Network
Plan Feature
Well Vision Exam $10 copay Up to $45
Single: up to $30
Bifocal: up to $50
Lenses/Prescription Glasses $25 copay
Trifocal: up to $60
Lenticular: up to $75
Frames $200 allowance + 20% off amount Up to $50
over allowance
Elective Contact Lens Care $160 allowance for contacts; fitting Up to $100
and evaluation up to $60 copay
Medically Necessary $25 Copay Up to $210
Contact Lens Care
Laser Vision Correction (contracted Average 15% off regular price or 5% Not covered
facilities only) off promotional price
Lens Enhancements
• Scratch Resistant Coatings $0 Copay N/A
• Anti-Reflective Coatings $25 Copay N/A
*You are eligible for all services once every calendar year
Visit Eyeconic.com – Virtually try on eyewear to choose your perfect fit!
Additional services using your VSP coverage can be found online at www.eyeconic.com! This site
can show you the latest deals and promotions on eyewear and contact lenses—keeping you in the
loop on all the newest brands, trends and styles available. There is even a virtual ‘dressing room’ to
try on your eyewear before you order!
No matter what kind of eye products you use now, or you might try in the future, we have you
covered. Eyeconic even makes it easy to apply insurance toward an online purchase, and includes
the option to utilize the expertise of our VSP© doctor network.
17 2022 Benefits Enrollment