Page 11 - Franklin Madison 2022 Benefits Guide
P. 11
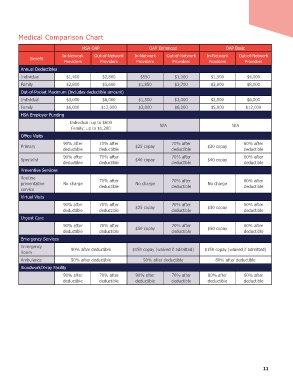
Medical Comparison Chart
HSA OAP OAP Enhanced OAP Basic
Beneit In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
Providers
Providers
Providers
Providers
Providers
Providers
Annual Deductibles
Individual $1,400 $2,800 $550 $1,100 $1,500 $4,000
Family $2,800 $5,600 $1,850 $3,700 $3,000 $8,000
Out-of-Pocket Maximum (Includes deductible amount)
Individual $3,000 $6,000 $1,500 $3,000 $2,500 $6,000
Family $6,000 $12,000 $3,000 $6,000 $5,000 $12,000
HSA Employer Funding
Individual: up to $600 N/A N/A
Family: up to $1,200
Oice Visits
60% after
70% after
Primary 90% after 70% after $25 copay deductible $30 copay deductible
deductible
deductible
70% after
60% after
Specialist 90% after 70% after $40 copay deductible $40 copay deductible
deductible
deductible
Preventive Services
Routine 70% after 70% after 60% after
preventative No charge deductible No charge deductible No charge deductible
service
Virtual Visits
90% after 70% after $25 copay 70% after $30 copay 60% after
deductible deductible deductible deductible
Urgent Care
90% after 70% after $50 copay 70% after $50 copay 60% after
deductible deductible deductible deductible
Emergency Services
Emergency 90% after deductible $150 copay (waived if admitted) $150 copay (waived if admitted)
Room
Ambulance 90% after deductible 90% after deductible 80% after deductible
Bloodwork/X-ray Facility
90% after 70% after 90% after 70% after 80% after 60% after
deductible deductible deductible deductible deductible deductible
11
HSA OAP OAP Enhanced OAP Basic
Beneit In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
Providers
Providers
Providers
Providers
Providers
Providers
Annual Deductibles
Individual $1,400 $2,800 $550 $1,100 $1,500 $4,000
Family $2,800 $5,600 $1,850 $3,700 $3,000 $8,000
Out-of-Pocket Maximum (Includes deductible amount)
Individual $3,000 $6,000 $1,500 $3,000 $2,500 $6,000
Family $6,000 $12,000 $3,000 $6,000 $5,000 $12,000
HSA Employer Funding
Individual: up to $600 N/A N/A
Family: up to $1,200
Oice Visits
60% after
70% after
Primary 90% after 70% after $25 copay deductible $30 copay deductible
deductible
deductible
70% after
60% after
Specialist 90% after 70% after $40 copay deductible $40 copay deductible
deductible
deductible
Preventive Services
Routine 70% after 70% after 60% after
preventative No charge deductible No charge deductible No charge deductible
service
Virtual Visits
90% after 70% after $25 copay 70% after $30 copay 60% after
deductible deductible deductible deductible
Urgent Care
90% after 70% after $50 copay 70% after $50 copay 60% after
deductible deductible deductible deductible
Emergency Services
Emergency 90% after deductible $150 copay (waived if admitted) $150 copay (waived if admitted)
Room
Ambulance 90% after deductible 90% after deductible 80% after deductible
Bloodwork/X-ray Facility
90% after 70% after 90% after 70% after 80% after 60% after
deductible deductible deductible deductible deductible deductible
11