
Page 5 - Florida Aquarium Benefits-at-a-Glance Guide 2022-2023
P. 5
Medical
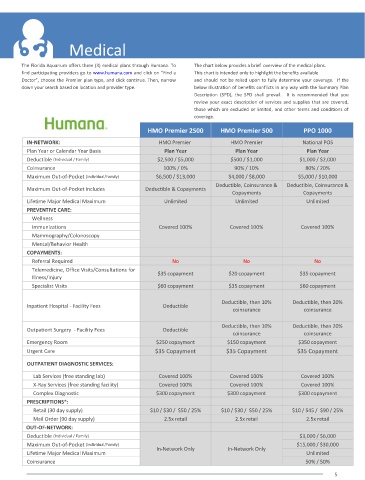
The Florida Aquarium offers three (3) medical plans through Humana. To The chart below provides a brief overview of the medical plans.
find participating providers go to www.humana.com and click on “Find a This chart is intended only to highlight the benefits available
Doctor”, choose the Premier plan type, and click continue. Then, narrow and should not be relied upon to fully determine your coverage. If the
down your search based on location and provider type. below illustration of benefits conflicts in any way with the Summary Plan
Description (SPD), the SPD shall prevail. It is recommended that you
review your exact description of services and supplies that are covered,
those which are excluded or limited, and other terms and conditions of
coverage.
HMO Premier 2500 HMO Premier 500 PPO 1000
IN-NETWORK: HMO Premier HMO Premier National POS
Plan Year or Calendar Year Basis Plan Year Plan Year Plan Year
Deductible (Individual / Family) $2,500 / $5,000 $500 / $1,000 $1,000 / $2,000
Coinsurance 100% / 0% 90% / 10% 80% / 20%
Maximum Out-of-Pocket (Individual/Family) $6,500 / $13,000 $4,000 / $8,000 $5,000 / $10,000
Deductible, Coinsurance & Deductible, Coinsurance &
Maximum Out-of-Pocket Includes Deductible & Copayments
Copayments Copayments
Lifetime Major Medical Maximum Unlimited Unlimited Unlimited
PREVENTIVE CARE:
Wellness
Immunizations Covered 100% Covered 100% Covered 100%
Mammography/Colonoscopy
Mental/Behavior Health
COPAYMENTS:
Referral Required No No No
Telemedicine, Office Visits/Consultations for
$35 copayment $20 copayment $35 copayment
Illness/Injury
Specialist Visits $60 copayment $35 copayment $60 copayment
Deductible, then 10% Deductible, then 20%
Inpatient Hospital - Facility Fees Deductible
coinsurance coinsurance
Deductible, then 10% Deductible, then 20%
Outpatient Surgery - Facility Fees Deductible
coinsurance coinsurance
Emergency Room $250 copayment $150 copayment $350 copayment
Urgent Care $35 Copayment $35 Copayment $35 Copayment
OUTPATIENT DIAGNOSTIC SERVICES:
Lab Services (free standing lab) Covered 100% Covered 100% Covered 100%
X-Ray Services (free standing facility) Covered 100% Covered 100% Covered 100%
Complex Diagnostic $300 copayment $300 copayment $300 copayment
PRESCRIPTIONS*:
Retail (30 day supply) $10 / $30 / $50 / 25% $10 / $30 / $50 / 25% $10 / $45 / $90 / 25%
Mail Order (90 day supply) 2.5x retail 2.5x retail 2.5x retail
OUT-OF-NETWORK:
Deductible (Individual / Family) $3,000 / $6,000
Maximum Out-of-Pocket (Individual/Family) $15,000 / $30,000
In-Network Only In-Network Only
Lifetime Major Medical Maximum Unlimited
Coinsurance 50% / 50%
5