
Page 5 - 2022 CAPREIT Benefits Guide
P. 5
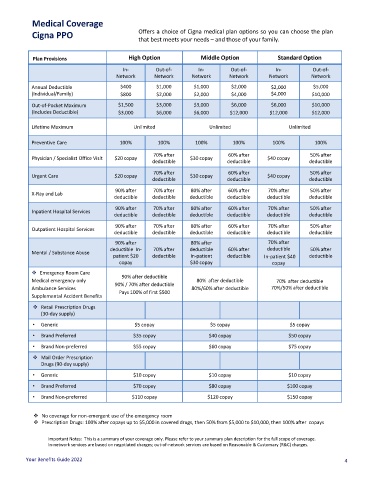
Medical Coverage
Cigna PPO Offers a choice of Cigna medical plan options so you can choose the plan
that best meets your needs – and those of your family.
Plan Provisions High Option Middle Option Standard Option
In- Out-of- In- Out-of- In- Out-of-
Network Network Network Network Network Network
Annual Deductible $400 $1,000 $1,000 $2,000 $2,000 $5,000
(Individual/Family) $800 $2,000 $2,000 $4,000 $4,000 $10,000
Out-of-Pocket Maximum $1,500 $3,000 $3,000 $6,000 $6,000 $10,000
(Includes Deductible) $3,000 $6,000 $6,000 $12,000 $12,000 $12,000
Lifetime Maximum Unlimited Unlimited Unlimited
Preventive Care 100% 100% 100% 100% 100% 100%
70% after 60% after 50% after
Physician / Specialist Office Visit $20 copay $30 copay $40 copay
deductible deductible deductible
70% after 60% after 50% after
Urgent Care $20 copay $30 copay $40 copay
deductible deductible deductible
90% after 70% after 80% after 60% after 70% after 50% after
X-Ray and Lab
deductible deductible deductible deductible deductible deductible
90% after 70% after 80% after 60% after 70% after 50% after
Inpatient Hospital Services
deductible deductible deductible deductible deductible deductible
90% after 70% after 80% after 60% after 70% after 50% after
Outpatient Hospital Services
deductible deductible deductible deductible deductible deductible
90% after 80% after 70% after
deductible In- 70% after deductible 60% after deductible 50% after
Mental / Substance Abuse
patient $20 deductible In-patient deductible In-patient $40 deductible
copay $30 copay copay
❖ Emergency Room Care
90% after deductible
Medical emergency only 80% after deductible 70% after deductible
90% / 70% after deductible
Ambulance Services 80%/60% after deductible 70%/50% after deductible
Pays 100% of first $500
Supplemental Accident Benefits
❖ Retail Prescription Drugs
(30-day supply)
• Generic $5 copay $5 copay $5 copay
• Brand Preferred $35 copay $40 copay $50 copay
• Brand Non-preferred $55 copay $60 copay $75 copay
❖ Mail Order Prescription
Drugs (90-day supply)
• Generic $10 copay $10 copay $10 copay
• Brand Preferred $70 copay $80 copay $100 copay
• Brand Non-preferred $110 copay $120 copay $150 copay
❖ No coverage for non-emergent use of the emergency room
❖ Prescription Drugs: 100% after copays up to $5,000 in covered drugs, then 50% from $5,000 to $10,000, then 100% after copays
Important Notes: This is a summary of your coverage only. Please refer to your summary plan description for the full scope of coverage.
In-network services are based on negotiated charges; out-of-network services are based on Reasonable & Customary (R&C) charges.
Your Benefits Guide 2022 4