
Page 7 - TimkenSteel 2022 Benefit Guide
P. 7
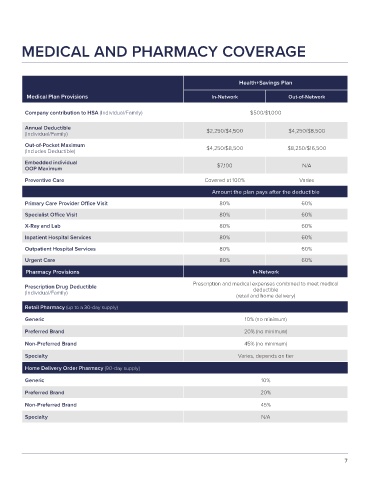
MEDICAL AND PHARMACY COVERAGE
Health+Savings Plan
Medical Plan Provisions In-Network Out-of-Network
Company contribution to HSA (Individual/Family) $500/$1,000
Annual Deductible
(Individual/Family) $2,250/$4,500 $4,250/$8,500
Out-of-Pocket Maximum
(Includes Deductible) $4,250/$8,500 $8,250/$16,500
Embedded individual
OOP Maximum $7,100 N/A
Preventive Care Covered at 100% Varies
Amount the plan pays after the deductible
Primary Care Provider Office Visit 80% 60%
Specialist Office Visit 80% 60%
X-Ray and Lab 80% 60%
Inpatient Hospital Services 80% 60%
Outpatient Hospital Services 80% 60%
Urgent Care 80% 60%
Pharmacy Provisions In-Network
Prescription Drug Deductible Prescription and medical expenses combined to meet medical
(Individual/Family) deductible
(retail and home delivery)
Retail Pharmacy (up to a 30-day supply)
Generic 10% (no minimum)
Preferred Brand 20% (no minimum)
Non-Preferred Brand 45% (no minimum)
Specialty Varies, depends on tier
Home Delivery Order Pharmacy (90-day supply)
Generic 10%
Preferred Brand 20%
Non-Preferred Brand 45%
Specialty N/A
7