
Page 5 - 2023 HCTec Benefits Guide Consultant
P. 5
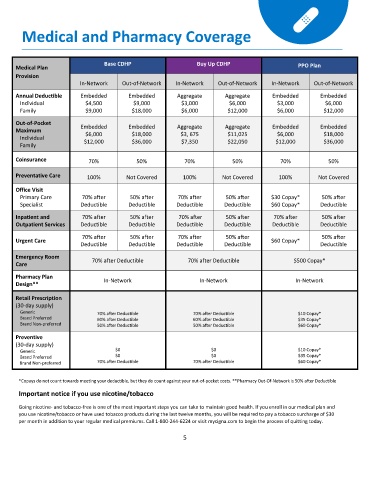
Medical and Pharmacy Coverage
Base CDHP Buy Up CDHP
Medical Plan PPO Plan
Provision
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
Annual Deductible Embedded Embedded Aggregate Aggregate Embedded Embedded
Individual $4,500 $9,000 $3,000 $6,000 $3,000 $6,000
Family $9,000 $18,000 $6,000 $12,000 $6,000 $12,000
Out-of-Pocket
Embedded Embedded Aggregate Aggregate Embedded Embedded
Maximum $6,000 $18,000 $3, 675 $11,025 $6,000 $18,000
Individual $12,000 $36,000 $7,350 $22,050 $12,000 $36,000
Family
Coinsurance 70% 50% 70% 50% 70% 50%
Preventative Care 100% Not Covered 100% Not Covered 100% Not Covered
Office Visit
Primary Care 70% after 50% after 70% after 50% after $30 Copay* 50% after
Specialist Deductible Deductible Deductible Deductible $60 Copay* Deductible
Inpatient and 70% after 50% after 70% after 50% after 70% after 50% after
Outpatient Services Deductible Deductible Deductible Deductible Deductible Deductible
70% after 50% after 70% after 50% after 50% after
Urgent Care $60 Copay*
Deductible Deductible Deductible Deductible Deductible
Emergency Room
70% after Deductible 70% after Deductible $500 Copay*
Care
Pharmacy Plan In-Network In-Network In-Network
Design**
Retail Prescription
(30-day supply)
Generic 70% after Deductible 70% after Deductible $10 Copay*
Brand Preferred 60% after Deductible 60% after Deductible $35 Copay*
Brand Non-preferred 50% after Deductible 50% after Deductible $60 Copay*
Preventive
(30-day supply)
Generic $0 $0 $10 Copay*
Brand Preferred $0 $0 $35 Copay*
Brand Non-preferred 70% after Deductible 70% after Deductible $60 Copay*
*Copays do not count towards meeting your deductible, but they do count against your out-of-pocket costs. **Pharmacy Out-Of-Network is 50% after Deductible
Important notice if you use nicotine/tobacco
Going nicotine- and tobacco-free is one of the most important steps you can take to maintain good health. If you enroll in our medical plan and
you use nicotine/tobacco or have used tobacco products during the last twelve months, you will be required to pay a tobacco surcharge of $30
per month in addition to your regular medical premiums. Call 1-800-244-6224 or visit mycigna.com to begin the process of quitting today.
5