
Page 6 - Immucor Benefit Guide
P. 6
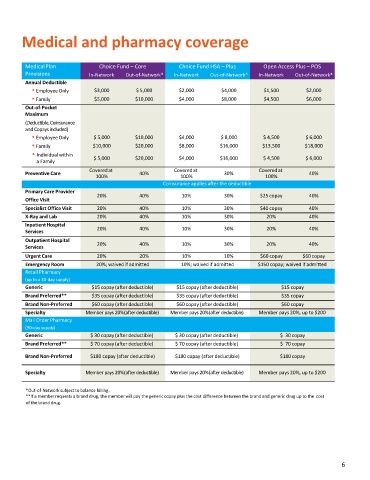
Medical and pharmacy coverage
MedicalPlan Choice Fund – Core Choice Fund HSA – Plus Open Access Plus – POS
Provisions In-Network Out-of-Network* In-Network Out-of-Network* In-Network Out-of-Network*
Annual Deductible
EmployeeOnly $3,000 $ 5,000 $2,000 $4,000 $1,500 $2,000
Family $5,000 $10,000 $4,000 $8,000 $4,500 $6,000
Out-of-Pocket
Maximum
(Deductible,Coinsurance
andCopaysincluded)
EmployeeOnly $ 5,000 $10,000 $4,000 $ 8,000 $ 4,500 $ 6,000
Family $10,000 $20,000 $8,000 $16,000 $13,500 $18,000
Individual within
a Family $ 5,000 $20,000 $4,000 $16,000 $ 4,500 $ 6,000
Coveredat Coveredat Coveredat
Preventive Care 40% 30% 40%
100% 100% 100%
Coinsurance applies after the deductible
Primary Care Provider
20% 40% 10% 30% $25 copay 40%
Office Visit
Specialist Office Visit 20% 40% 10% 30% $40 copay 40%
X-Ray and Lab 20% 40% 10% 30% 20% 40%
InpatientHospital
Services 20% 40% 10% 30% 20% 40%
Outpatient Hospital
20% 40% 10% 30% 20% 40%
Services
Urgent Care 20% 20% 10% 10% $60 copay $60 copay
Emergency Room 20%; waived if admitted 10%; waived if admitted $150 copay; waived if admitted
Retail Pharmacy
(up to a 30-day supply)
Generic $15 copay (after deductible) $15 copay (after deductible) $15 copay
Brand Preferred** $35 copay (after deductible) $35 copay (after deductible) $35 copay
Brand Non-Preferred $60 copay (after deductible) $60 copay (after deductible) $60 copay
Specialty Member pays 20%(after deductible) Member pays 20%(after deductible) Member pays 20%, up to $200
Mail Order Pharmacy
(90-day supply)
Generic $ 30 copay (after deductible) $ 30 copay (after deductible) $ 30 copay
Brand Preferred** $ 70 copay (after deductible) $ 70 copay (after deductible) $ 70 copay
Brand Non-Preferred $180 copay (after deductible) $180 copay (after deductible) $180 copay
Specialty Member pays 20%(after deductible) Member pays 20%(after deductible) Member pays 20%, up to $200
*Out-of-Network subject to balance billing.
**If a member requests a brand drug, the member will pay the generic copay plus the cost difference between the brand and generic drug up to the cost
of the brand drug.
6