
Page 6 - 2022 Fives Landis Corp Benefit Guide
P. 6
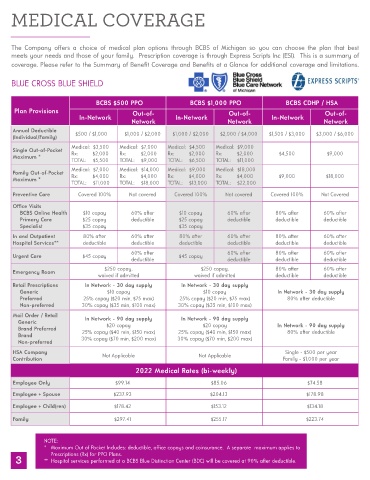
MEDICAL COVERAGE
The Company offers a choice of medical plan options through BCBS of Michigan so you can choose the plan that best
meets your needs and those of your family. Prescription coverage is through Express Scripts Inc (ESI). This is a summary of
coverage. Please refer to the Summary of Benefit Coverage and Benefits at a Glance for additional coverage and limitations.
BLUE CROSS BLUE SHIELD
BCBS $500 PPO BCBS $1,000 PPO BCBS CDHP / HSA
Plan Provisions Out-of- Out-of- Out-of-
In-Network In-Network In-Network
Network Network Network
Annual Deductible $500 / $1,000 $1,000 / $2,000 $1,000 / $2,000 $2,000 / $4,000 $1,500 / $3,000 $3,000 / $6,000
(Individual/Family)
Medical: $3,500 Medical: $7,000 Medical: $4,500 Medical: $9,000
Single Out-of-Pocket
Maximum * Rx: $2,000 Rx: $2,000 Rx: $2,000 Rx: $2,000 $4,500 $9,000
TOTAL: $5,500 TOTAL: $9,000 TOTAL: $6,500 TOTAL: $11,000
Medical: $7,000 Medical: $14,000 Medical: $9,000 Medical: $18,000
Family Out-of-Pocket
Maximum * Rx: $4,000 Rx: $4,000 Rx: $4,000 Rx: $4,000 $9,000 $18,000
TOTAL: $11,000 TOTAL: $18,000 TOTAL: $13,000 TOTAL: $22,000
Preventive Care Covered 100% Not covered Covered 100% Not covered Covered 100% Not Covered
Office Visits
BCBS Online Health $10 copay 60% after $10 copay 60% after 80% after 60% after
Primary Care $25 copay deductible $25 copay deductible deductible deductible
Specialist $35 copay $35 copay
In and Outpatient 80% after 60% after 80% after 60% after 80% after 60% after
Hospital Services** deductible deductible deductible deductible deductible deductible
60% after 60% after 80% after 60% after
Urgent Care $45 copay $45 copay
deductible deductible deductible deductible
$250 copay, $250 copay, 80% after 60% after
Emergency Room
waived if admitted waived if admitted deductible deductible
Retail Prescriptions In Network - 30 day supply In Network - 30 day supply
Generic $10 copay $10 copay In Network - 30 day supply
Preferred 25% copay ($20 min, $75 max) 25% copay ($20 min, $75 max) 80% after deductible
Non-preferred 30% copay ($35 min, $100 max) 30% copay ($35 min, $100 max)
Mail Order / Retail In Network - 90 day supply In Network - 90 day supply
Generic $20 copay $20 copay In Network - 90 day supply
Brand Preferred 25% copay ($40 min, $150 max) 25% copay ($40 min, $150 max) 80% after deductible
Brand 30% copay ($70 min, $200 max) 30% copay ($70 min, $200 max)
Non-preferred
HSA Company Single - $500 per year
Contribution Not Applicable Not Applicable Family - $1,000 per year
2022 Medical Rates (bi-weekly)
Employee Only $99.14 $85.06 $74.58
Employee + Spouse $237.93 $204.13 $178.98
Employee + Child(ren) $178.42 $153.12 $134.18
Family $297.41 $255.17 $223.74
NOTE:
* Maximum Out of Pocket Includes: deductible, office copays and coinsurance. A separate maximum applies to
3 Prescriptions (Rx) for PPO Plans.
** Hospital services performed at a BCBS Blue Distinction Center (BDC) will be covered at 90% after deductible.