
Page 7 - 2022-23 Drug Plastics Benefit Guide
P. 7
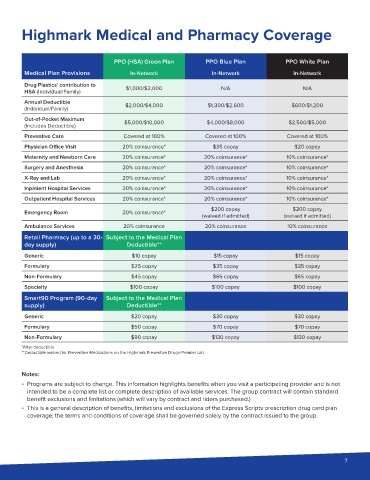
Highmark Medical and Pharmacy Coverage
PPO (HSA) Green Plan PPO Blue Plan PPO White Plan
Medical Plan Provisions In-Network In-Network In-Network
Drug Plastics’ contribution to $1,000/$2,000 N/A N/A
HSA (Individual/Family)
Annual Deductible
(Individual/Family) $2,000/$4,000 $1,300/$2,600 $600/$1,200
Out-of-Pocket Maximum
(Includes Deductible) $5,000/$10,000 $4,000/$8,000 $2,500/$5,000
Preventive Care Covered at 100% Covered at 100% Covered at 100%
Physician Office Visit 20% coinsurance* $35 copay $20 copay
Maternity and Newborn Care 20% coinsurance* 20% coinsurance* 10% coinsurance*
Surgery and Anesthesia 20% coinsurance* 20% coinsurance* 10% coinsurance*
X-Ray and Lab 20% coinsurance* 20% coinsurance* 10% coinsurance*
Inpatient Hospital Services 20% coinsurance* 20% coinsurance* 10% coinsurance*
Outpatient Hospital Services 20% coinsurance* 20% coinsurance* 10% coinsurance*
$200 copay $200 copay
Emergency Room 20% coinsurance*
(waived if admitted) (waived if admitted)
Ambulance Services 20% coinsurance 20% coinsurance 10% coinsurance
Retail Pharmacy (up to a 30- Subject to the Medical Plan
day supply) Deductible**
Generic $10 copay $15 copay $15 copay
Formulary $25 copay $35 copay $35 copay
Non-Formulary $45 copay $65 copay $65 copay
Specialty $100 copay $100 copay $100 copay
Smart90 Program (90-day Subject to the Medical Plan
supply) Deductible**
Generic $20 copay $30 copay $30 copay
Formulary $50 copay $70 copay $70 copay
Non-Formulary $90 copay $130 copay $130 copay
*After deductible
**Deductible waived for Preventive Medications on the Highmark Preventive Drugs-Premier List
Notes:
΅ Programs are subject to change. This information highlights benefits when you visit a participating provider and is not
intended to be a complete list or complete description of available services. The group contract will contain standard
benefit exclusions and limitations (which will vary by contract and riders purchased.)
΅ This is a general description of benefits, limitations and exclusions of the Express Scripts prescription drug card plan
coverage; the terms and conditions of coverage shall be governed solely by the contract issued to the group.
7