
Page 5 - Fort Health Care 2022 Benefit Guide
P. 5
5 | P a g e
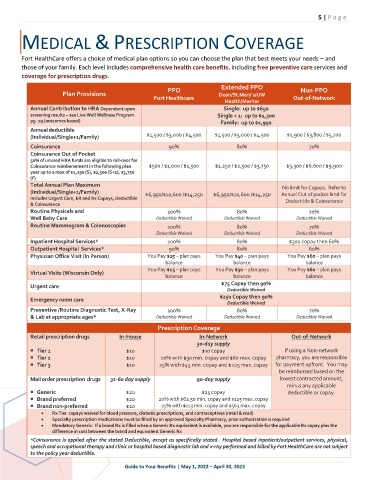
MEDICAL & PRESCRIPTION COVERAGE
Fort HealthCare offers a choice of medical plan options so you can choose the plan that best meets your needs – and
those of your family. Each level includes comprehensive health care benefits, including free preventive care services and
coverage for prescription drugs.
Extended PPO
PPO Non-PPO
Plan Provisions Dean/St.Mary’s/UW
Fort Healthcare Out-of-Network
Health/Meriter
Annual Contribution to HRA Dependent upon Single: up to $650
screening results – see Live Well Wellness Program Single + 1: up to $1,300
pg. 19 (outcomes based) Family: up to $1,950
Annual deductible
$1,500 / $3,000 / $4,500 $1,500 / $3,000 / $4,500 $1,900 / $3,800 / $5,700
(Individual/Single+1/Family)
Coinsurance 90% 80% 70%
Coinsurance Out of Pocket
50% of unused HRA funds are eligible to roll-over for
Coinsurance reimbursement in the following plan $500 / $1,000 / $1,500 $1,250 / $2,500 / $3,750 $3,300 / $6,600 / $9,900
year up to a max of $1,250 (S), $2,500 (S+1), $3,750
(F)
Total Annual Plan Maximum
No limit for Copays. Refer to
(Individual/Single+1/Family) $6,950/$10,600 /$14,250 $6,950/$10,600 /$14,250 Annual Out of pocket limit for
Includes Urgent Care, ER and Rx Copays, Deductible Deductible & Coinsurance
& Coinsurance
Routine Physicals and 100% 80% 70%
Well Baby Care Deductible Waived Deductible Waived Deductible Waived
Routine Mammogram & Colonoscopies 100% 80% 70%
Deductible Waived Deductible Waived Deductible Waived
Inpatient Hospital Services* 100% 80% $300 copay then 60%
Outpatient Hospital Services* 90% 80% 60%
Physician Office Visit (In Person) You Pay $25 – plan pays You Pay $40 – plan pays You Pay $60 – plan pays
balance balance balance
You Pay $15 – plan pays You Pay $30 – plan pays You Pay $60 – plan pays
Virtual Visits (Wisconsin Only)
balance balance balance
$75 Copay then 90%
Urgent care
Deductible Waived
$250 Copay then 90%
Emergency room care
Deductible Waived
Preventive /Routine Diagnostic Test, X-Ray 100% 80% 70%
& Lab at appropriate ages* Deductible Waived Deductible Waived Deductible Waived
Prescription Coverage
Retail prescription drugs In-House In-Network Out-of-Network
30-day supply
Tier 1 $10 $10 copay If using a Non-network
Tier 2 $10 20% with $30 min. copay and $60 max. copay pharmacy, you are responsible
Tier 3 $10 25% with $45 min. copay and $225 max. copay for payment upfront. You may
be reimbursed based on the
Mail order prescription drugs 31-60 day supply 90-day supply lowest contracted amount,
minus any applicable
Generic $20 $25 copay deductible or copay.
Brand preferred $20 20% with $62.50 min. copay and $125 max. copay
Brand non-preferred $20 25% with $113 min. copay and $563 max. copay
• Rx Tier copays waived for blood pressure, diabetic prescriptions, and contraceptives (retail & mail)
• Specialty prescription medications must be filled by an approved Specialty Pharmacy, prior authorization is required
• Mandatory Generic: If a brand Rx is filled when a Generic Rx equivalent is available, you are responsible for the applicable Rx copay plus the
difference in cost between the brand and equivalent Generic Rx
*Coinsurance is applied after the stated Deductible, except as specifically stated. Hospital based inpatient/outpatient services, physical,
speech and occupational therapy and clinic or hospital based diagnostic lab and x-ray performed and billed by Fort HealthCare are not subject
to the policy year deductible.
Guide to Your Benefits | May 1, 2022 – April 30, 2023