
Page 7 - 2021 Marcolin Benefit Guide
P. 7
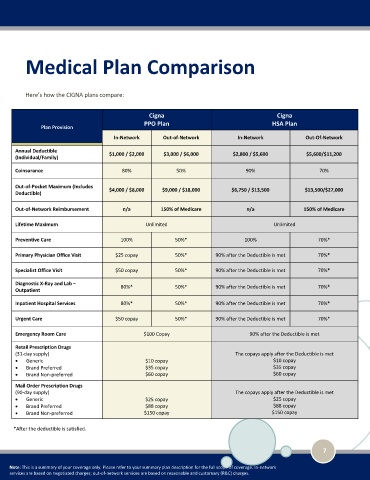
Medical Plan Comparison
Here’s how the CIGNA plans compare:
Cigna Cigna
PPO Plan HSA Plan
Plan Provision
In-Network Out-of-Network In-Network Out-Of-Network
Annual Deductible $1,000 / $2,000 $3,000 / $6,000 $2,800 / $5,600 $5,600/$11,200
(Individual/Family)
Coinsurance 80% 50% 90% 70%
Out-of-Pocket Maximum (Includes $4,000 / $8,000 $9,000 / $18,000 $6,750 / $13,500 $13,500/$27,000
Deductible)
Out-of-Network Reimbursement n/a 150% of Medicare n/a 150% of Medicare
Lifetime Maximum Unlimited Unlimited
Preventive Care 100% 50%* 100% 70%*
Primary Physician Office Visit $25 copay 50%* 90% after the Deductible is met 70%*
Specialist Office Visit $50 copay 50%* 90% after the Deductible is met 70%*
Diagnostic X-Ray and Lab – 80%* 50%* 90% after the Deductible is met 70%*
Outpatient
Inpatient Hospital Services 80%* 50%* 90% after the Deductible is met 70%*
Urgent Care $50 copay 50%* 90% after the Deductible is met 70%*
Emergency Room Care $100 Copay 90% after the Deductible is met
Retail Prescription Drugs
(31-day supply) The copays apply after the Deductible is met
• Generic $10 copay $10 copay
• Brand Preferred $35 copay $35 copay
• Brand Non-preferred $60 copay $60 copay
Mail Order Prescription Drugs
(90-day supply) The copays apply after the Deductible is met
• Generic $25 copay $25 copay
• Brand Preferred $88 copay $88 copay
• Brand Non-preferred $150 copay $150 copay
*After the deductible is satisfied.
7
Note: This is a summary of your coverage only. Please refer to your summary plan description for the full scope of coverage. In-network
services are based on negotiated charges; out-of-network services are based on reasonable and customary (R&C) charges.