
Page 4 - 2026 Affinity Neurocare Benefit Guide Final v2
P. 4
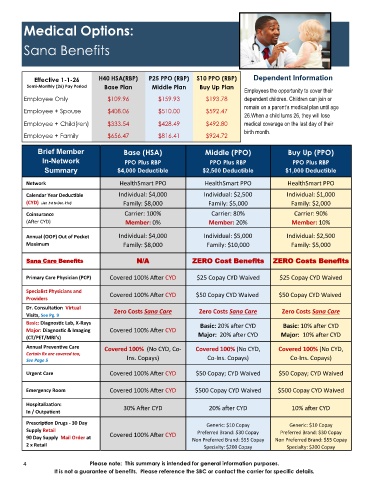
Medical Options:
Sana Benefits
Effective 1-1-26 H40 HSA(RBP) P25 PPO (RBP) S10 PPO (RBP) Dependent Information
Semi-Monthly (26) Pay Period Base Plan Middle Plan Buy Up Plan
Employees the opportunity to cover their
Employee Only $109.96 $159.93 $193.78 dependent children. Children can join or
remain on a parent’s medical plan until age
Employee + Spouse $408.06 $510.00 $592.47
26.When a child turns 26, they will lose
Employee + Child(ren) $333.54 $428.49 $492.80 medical coverage on the last day of their
birth month.
Employee + Family $656.47 $816.41 $924.72
Brief Member Base (HSA) Middle (PPO) Buy Up (PPO)
In-Network PPO Plus RBP PPO Plus RBP PPO Plus RBP
Summary $4,000 Deductible $2,500 Deductible $1,000 Deductible
Network HealthSmart PPO HealthSmart PPO HealthSmart PPO
Calendar Year Deductible Individual: $4,000 Individual: $2,500 Individual: $1,000
Family: $8,000 Family: $5,000 Family: $2,000
(CYD) (Jan .1st to Dec. 31st)
Coinsurance Carrier: 100% Carrier: 80% Carrier: 90%
(After CYD) Member: 0% Member: 20% Member: 10%
Annual (OOP) Out of Pocket Individual: $4,000 Individual: $5,000 Individual: $2,500
Maximum Family: $8,000 Family: $10,000 Family: $5,000
Sana Care Benefits N/A ZERO Cost Benefits ZERO Costs Benefits
Primary Care Physician (PCP) Covered 100% After CYD $25 Copay CYD Waived $25 Copay CYD Waived
Specialist Physicians and
Covered 100% After CYD $50 Copay CYD Waived $50 Copay CYD Waived
Providers
Dr. Consultation Virtual
Zero Costs Sana Care Zero Costs Sana Care Zero Costs Sana Care
Visits, See Pg. 9
Basic: Diagnostic Lab, X-Rays Basic: 20% after CYD Basic: 10% after CYD
Major: Diagnostic & Imaging Covered 100% After CYD
(CT/PET/MRI’s) Major: 20% after CYD Major: 10% after CYD
Annual Preventive Care Covered 100% (No CYD, Co- Covered 100% (No CYD, Covered 100% (No CYD,
Certain Rx are covered too,
See Page 5 Ins. Copays) Co-Ins. Copays) Co-Ins. Copays)
Urgent Care Covered 100% After CYD $50 Copay; CYD Waived $50 Copay; CYD Waived
Emergency Room Covered 100% After CYD $500 Copay CYD Waived $500 Copay CYD Waived
Hospitalization: 30% After CYD 20% after CYD 10% after CYD
In / Outpatient
Prescription Drugs - 30 Day Generic: $10 Copay Generic: $10 Copay
Supply Retail Preferred Brand: $30 Copay
Preferred Brand: $30 Copay
90 Day Supply Mail Order at Covered 100% After CYD Non Preferred Brand: $55 Copay Non Preferred Brand: $55 Copay
2 x Retail Specialty: $200 Copay Specialty: $200 Copay
4 Please note: This summary is intended for general information purposes.
It is not a guarantee of benefits. Please reference the SBC or contact the carrier for specific details.