
Page 9 - Affinity Neurocare Benefit Guide 2022 updated
P. 9
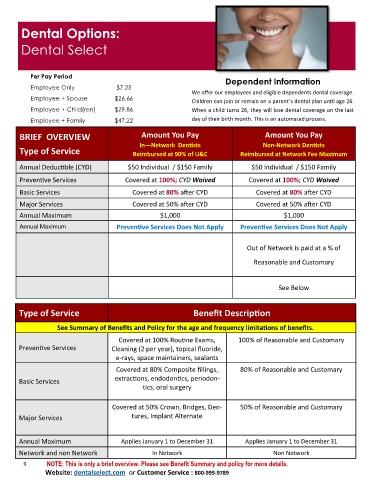
Dental Options:
Dental Select
Per Pay Period Dependent Information
Employee Only $7.25
We offer our employees and eligible dependents dental coverage.
Employee + Spouse $26.66
Children can join or remain on a parent’s dental plan until age 26.
Employee + Child(ren) $29.86 When a child turns 26, they will lose dental coverage on the last
Employee + Family $47.22 day of their birth month. This is an automated process.
BRIEF OVERVIEW Amount You Pay Amount You Pay
In—Network Dentists Non-Network Dentists
Type of Service Reimbursed at 90% of U&C Reimbursed at Network Fee Maximum
Annual Deductible (CYD) $50 Individual / $150 Family $50 Individual / $150 Family
Preventive Services Covered at 100%; CYD Waived Covered at 100%; CYD Waived
Basic Services Covered at 80% after CYD Covered at 80% after CYD
Major Services Covered at 50% after CYD Covered at 50% after CYD
Annual Maximum $1,000 $1,000
Annual Maximum Preventive Services Does Not Apply Preventive Services Does Not Apply
Out of Network is paid at a % of
Reasonable and Customary
See Below
Type of Service Benefit Description
See Summary of Benefits and Policy for the age and frequency limitations of benefits.
Covered at 100% Routine Exams, 100% of Reasonable and Customary
Preventive Services Cleaning (2 per year), topical fluoride,
e-rays, space maintainers, sealants
Covered at 80% Composite fillings, 80% of Reasonable and Customary
extractions, endodontics, periodon-
Basic Services
tics, oral surgery
Covered at 50% Crown, Bridges, Den- 50% of Reasonable and Customary
Major Services tures, Implant Alternate
Annual Maximum Applies January 1 to December 31 Applies January 1 to December 31
Network and non Network In Network Non Network
9 NOTE: This is only a brief overview. Please see Benefit Summary and policy for more details.
Website: dentalselect.com or Customer Service : 800-999-9789