
Page 4 - Affinity Neurocare Benefit Guide 2022 updated
P. 4
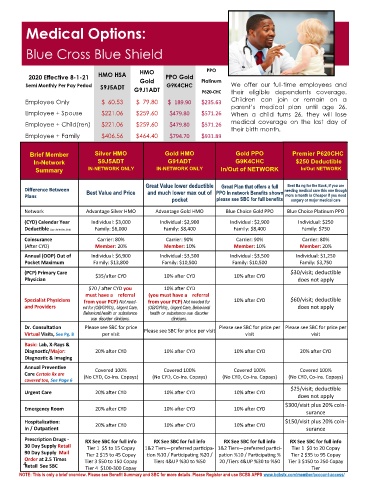
Medical Options:
Blue Cross Blue Shield
PPO
2020 Effective 8-1-21 HMO HSA HMO PPO Gold Platinum
Gold
Semi Monthly Per Pay Period S9J5ADT G9J1ADT G9K4CHC P620-CHC We offer our full-time employees and
their eligible dependents coverage.
Employee Only $ 60.53 $ 79.80 $ 189.90 $235.63 Children can join or remain on a
parent’s medical plan until age 26.
Employee + Spouse $221.06 $259.60 $479.80 $571.26 When a child turns 26, they will lose
Employee + Child(ren) $221.06 $259.60 $479.80 $571.26 medical coverage on the last day of
their birth month.
Employee + Family $406.56 $464.40 $794.70 $931.89
Brief Member Silver HMO Gold HMO Gold PPO Premier P620CHC
In-Network S9J5ADT G91ADT G9K4CHC $250 Deductible
Summary IN-NETWORK ONLY IN-NETWORK ONLY In/Out of NETWORK In/Out NETWORK
Great Value lower deductible Great Plan that offers a full Best Ba ng for the Buck, if you are
Difference Between Best Value and Price and much lower max out of PPO In network Benefits shown needing medical care this one though
Plans more a month is Cheaper if you need
pocket please see SBC for full benefits surgery or major medical care
Network Advantage Silver HMO Advantage Gold HMO Blue Choice Gold PPO Blue Choice Platinum PPO
(CYD) Calendar Year Individual: $3,000 Individual: $2,900 Individual: $2,900 Individual: $250
Family: $6,000 Family: $8,400 Family: $8,400 Family: $750
Deductible (Jan .1st to Dec. 31st)
Coinsurance Carrier: 80% Carrier: 90% Carrier: 90% Carrier: 80%
(After CYD) Member: 20% Member: 10% Member: 10% Member: 20%
Annual (OOP) Out of Individual: $6,900 Individual: $3,500 Individual: $3,500 Individual: $1,250
Pocket Maximum Family: $13,800 Family: $10,500 Family: $10,500 Family: $3,750
(PCP) Primary Care $35/after CYD 10% after CYD 10% after CYD $30/visit; deductible
Physician does not apply
$70 / after CYD you 10% after CYD
must have a referral (you must have a referral
Specialist Physicians from your PCP) Not need- from your PCP) Not needed for 10% after CYD $60/visit; deductible
and Providers ed for (OB/GYN’s)., Urgent Care, (OB/GYN’s)., Urgent Care, Behavioral does not apply
Behavioral health or health or use disorder
use disorder clinicians. clinicians.
Dr. Consultation Please see SBC for price Please see SBC for price per visit Please see SBC for price per Please see SBC for price per
Virtual Visits, See Pg. 8 per visit visit visit
Basic: Lab, X-Rays &
Diagnostic/Major: 20% after CYD 10% after CYD 10% after CYD 20% after CYD
Diagnostic & Imaging
Annual Preventive
Covered 100% Covered 100% Covered 100% Covered 100%
Care Certain Rx are (No CYD, Co-Ins. Copays) (No CYD, Co-Ins. Copays) (No CYD, Co-Ins. Copays) (No CYD, Co-Ins. Copays)
covered too, See Page 6
$25/visit; deductible
Urgent Care 20% after CYD 10% after CYD 10% after CYD
does not apply
$300/visit plus 20% coin-
Emergency Room 20% after CYD 10% after CYD 10% after CYD
surance
Hospitalization: 20% after CYD 10% after CYD 10% after CYD $150/visit plus 20% coin-
In / Outpatient surance
Prescription Drugs - RX See SBC for full info RX See SBC for full info RX See SBC for full info RX See SBC for full info
30 Day Supply Retail Tier 1 $5 to 15 Copay referred participa- 1&2 Tiers—preferred partici- Tier 1 $0 to 20 Copay
—
p
1&2 T
e
i
rs
90 Day Supply Mail Tier 2 $15 to 45 Copay articipating %20 / pation %10 / Participating % Tier 2 $35 to 95 Copay
n
o
ti
%
10 / P
Order at 2.5 Times Tier 3 $50 to 150 Copay Tiers 4&UP %30 to %50 20 /Tiers 4&UP %30 to %50 Tier 3 $150 to 250 Copay
4 Tier 4 $100-300 Copay Tier
Retail See SBC
NOTE: This is only a brief overview. Please see Benefit Summary and SBC for more details. Please Register and use BCBS APPS www.bcbstx.com/member/account-access/