
Page 7 - Winsight 2021 Benefit Guide
P. 7
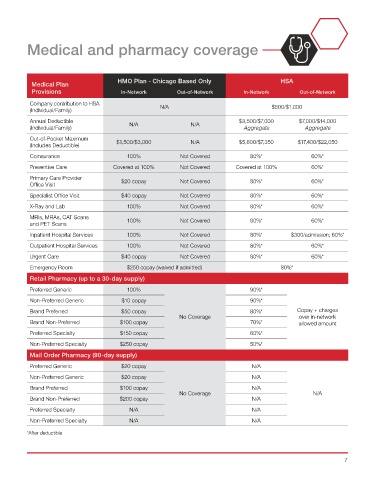
Medical and pharmacy coverage
HMO Plan - Chicago Based Only HSA
Medical Plan
Provisions In-Network Out-of-Network In-Network Out-of-Network
Company contribution to HSA
(Individual/Family) N/A $500/$1,000
Annual Deductible $3,500/$7,000 $7,000/$14,000
(Individual/Family) N/A N/A Aggregate Aggregate
Out-of-Pocket Maximum
(Includes Deductible) $1,500/$3,000 N/A $5,800/$7,350 $17,400/$22,050
Coinsurance 100% Not Covered 80%* 60%*
Preventive Care Covered at 100% Not Covered Covered at 100% 60%*
Primary Care Provider
Office Visit $20 copay Not Covered 80%* 60%*
Specialist Office Visit $40 copay Not Covered 80%* 60%*
X-Ray and Lab 100% Not Covered 80%* 60%*
MRIs, MRAs, CAT Scans 100% Not Covered 80%* 60%*
and PET Scans
Inpatient Hospital Services 100% Not Covered 80%* $300/admission; 60%*
Outpatient Hospital Services 100% Not Covered 80%* 60%*
Urgent Care $40 copay Not Covered 80%* 60%*
Emergency Room $250 copay (waived if admitted) 80%*
Retail Pharmacy (up to a 30-day supply)
Preferred Generic 100% 90%*
Non-Preferred Generic $10 copay 90%*
Brand Preferred $50 copay 80%* Copay + charges
No Coverage over in-network
Brand Non-Preferred $100 copay 70%* allowed amount
Preferred Specialty $150 copay 60%*
Non-Preferred Specialty $250 copay 50%*
Mail Order Pharmacy (90-day supply)
Preferred Generic $20 copay N/A
Non-Preferred Generic $20 copay N/A
Brand Preferred $100 copay N/A
No Coverage N/A
Brand Non-Preferred $200 copay N/A
Preferred Specialty N/A N/A
Non-Preferred Specialty N/A N/A
*After deductible
7