
Page 7 - HWS 2021 Benefit Guide
P. 7
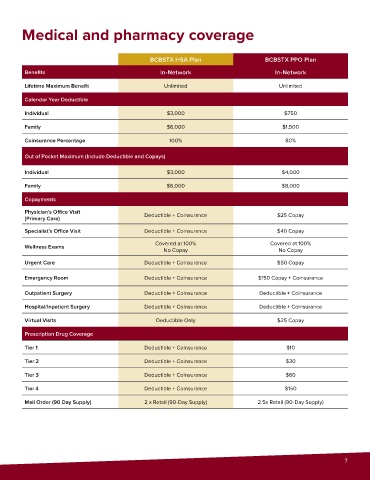
Medical and pharmacy coverage
BCBSTX HSA Plan BCBSTX PPO Plan
Benefits In-Network In-Network
Lifetime Maximum Benefit Unlimited Unlimited
Calendar Year Deductible
Individual $3,000 $750
Family $6,000 $1,500
Coinsurance Percentage 100% 80%
Out of Pocket Maximum (Include Deductible and Copays)
Individual $3,000 $4,000
Family $6,000 $8,000
Copayments
Physician's Office Visit
(Primary Care) Deductible + Coinsurance $25 Copay
Specialist's Office Visit Deductible + Coinsurance $40 Copay
Covered at 100% Covered at 100%
Wellness Exams
No Copay No Copay
Urgent Care Deductible + Coinsurance $50 Copay
Emergency Room Deductible + Coinsurance $150 Copay + Coinsurance
Outpatient Surgery Deductible + Coinsurance Deductible + Coinsurance
Hospital/Inpatient Surgery Deductible + Coinsurance Deductible + Coinsurance
Virtual Visits Deductible Only $25 Copay
Prescription Drug Coverage
Tier 1 Deductible + Coinsurance $10
Tier 2 Deductible + Coinsurance $30
Tier 3 Deductible + Coinsurance $60
Tier 4 Deductible + Coinsurance $150
Mail Order (90 Day Supply) 2 x Retail (90-Day Supply) 2.5x Retail (90-Day Supply)
7