
Page 3 - 2021 Open Sky Employee Benefits - SALARIED
P. 3
12/1/2020-11/30/2021 Employee Benefits Brochure
Salaried
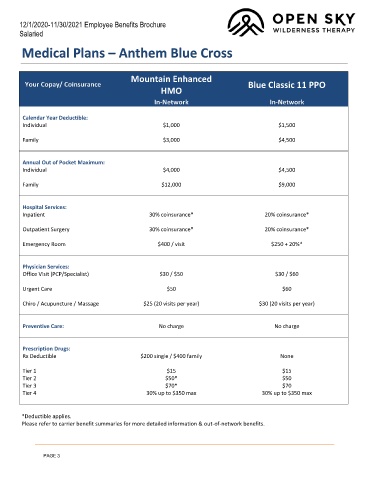
Medical Plans – Anthem Blue Cross
Mountain Enhanced
Your Copay/ Coinsurance Blue Classic 11 PPO
HMO
In-Network In-Network
Calendar Year Deductible:
Individual $1,000 $1,500
Family $3,000 $4,500
Annual Out of Pocket Maximum:
Individual $4,000 $4,500
Family $12,000 $9,000
Hospital Services:
Inpatient 30% coinsurance* 20% coinsurance*
Outpatient Surgery 30% coinsurance* 20% coinsurance*
Emergency Room $400 / visit $250 + 20%*
Physician Services:
Office Visit (PCP/Specialist) $30 / $50 $30 / $60
Urgent Care $50 $60
Chiro / Acupuncture / Massage $25 (20 visits per year) $30 (20 visits per year)
Preventive Care: No charge No charge
Prescription Drugs:
Rx Deductible $200 single / $400 family None
Tier 1 $15 $15
Tier 2 $50* $50
Tier 3 $70* $70
Tier 4 30% up to $350 max 30% up to $350 max
*Deductible applies.
Please refer to carrier benefit summaries for more detailed information & out-of-network benefits.
PAGE 3