
Page 5 - 2021 Open Sky Employee Benefits - SALARIED
P. 5
12/1/2020-11/30/2021 Employee Benefits Brochure
Salaried
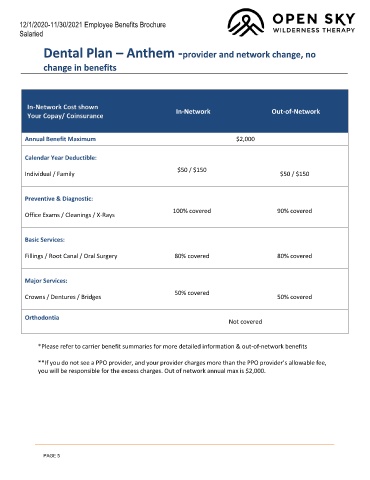
Dental Plan – Anthem -provider and network change, no
change in benefits
In-Network Cost shown
In-Network Out-of-Network
Your Copay/ Coinsurance
Annual Benefit Maximum $2,000
Calendar Year Deductible:
$50 / $150
Individual / Family $50 / $150
Preventive & Diagnostic:
100% covered 90% covered
Office Exams / Cleanings / X-Rays
Basic Services:
Fillings / Root Canal / Oral Surgery 80% covered 80% covered
Major Services:
50% covered
Crowns / Dentures / Bridges 50% covered
Orthodontia
Not covered
*Please refer to carrier benefit summaries for more detailed information & out-of-network benefits
**If you do not see a PPO provider, and your provider charges more than the PPO provider’s allowable fee,
you will be responsible for the excess charges. Out of network annual max is $2,000.
PAGE 5