
Page 5 - 2021-22 Velocity Employee Benefits Brochure
P. 5
Velocity Mortgage Capital
2021–2022 Employee Benefits Brochure
Medical Plans
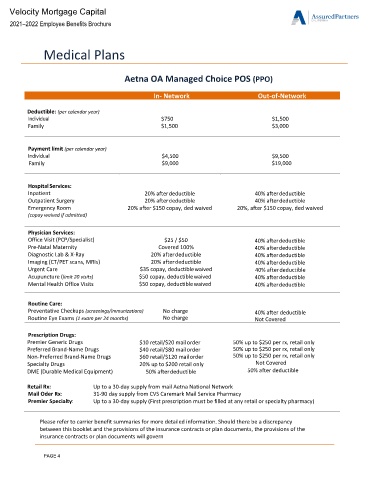
Aetna OA Managed Choice POS (PPO)
In- Network Out-of-Network
Deductible: (per calendar year)
Individual $750 $1,500
Family $1,500 $3,000
Payment limit (per calendar year)
Individual $4,500 $9,500
Family $9,000 $19,000
Hospital Services:
Inpatient 20% after deductible 40% after deductible
Outpatient Surgery 20% after deductible 40% after deductible
Emergency Room 20% after $150 copay, ded waived 20%, after $150 copay, ded waived
(copay waived if admitted)
Physician Services:
Office Visit (PCP/Specialist) $25 / $50 40% after deductible
Pre-Natal Maternity Covered 100% 40% after deductible
Diagnostic Lab & X-Ray 20% after deductible 40% after deductible
Imaging (CT/PET scans, MRIs) 20% after deductible 40% after deductible
Urgent Care $35 copay, deductible waived 40% after deductible
Acupuncture (limit 20 visits) $50 copay, deductible waived 40% after deductible
Mental Health Office Visits $50 copay, deductible waived 40% after deductible
Routine Care:
Preventative Checkups (screenings/immunizations) No charge 40% after deductible
Routine Eye Exams (1 exam per 24 months) No charge Not Covered
Prescription Drugs:
Premier Generic Drugs $10 retail/$20 mail order 50% up to $250 per rx, retail only
Preferred Brand-Name Drugs $40 retail/$80 mail order 50% up to $250 per rx, retail only
Non-Preferred Brand-Name Drugs $60 retail/$120 mail order 50% up to $250 per rx, retail only
Specialty Drugs 20% up to $200 retail only Not Covered
DME (Durable Medical Equipment) 50% after deductible 50% after deductible
Retail Rx: Up to a 30-day supply from mail Aetna National Network
Mail Oder Rx: 31-90 day supply from CVS Caremark Mail Service Pharmacy
Premier Specialty: Up to a 30-day supply (First prescription must be filled at any retail or specialty pharmacy)
Please refer to carrier benefit summaries for more detailed information. Should there be a discrepancy
between this booklet and the provisions of the insurance contracts or plan documents, the provisions of the
insurance contracts or plan documents will govern
PAGE 4