
Page 7 - 2021-22 Velocity Employee Benefits Brochure
P. 7
Velocity Mortgage Capital
2021–2022 Employee Benefits Brochure
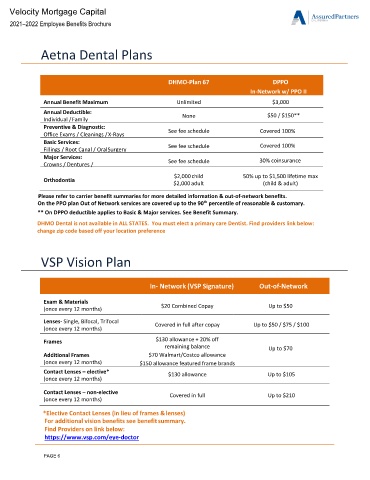
Aetna Dental Plans
DHMO-Plan 67 DPPO
In-Network w/ PPO II
Annual Benefit Maximum Unlimited $3,000
Annual Deductible:
Individual / Family None $50 / $150**
Preventive & Diagnostic:
Office Exams / Cleanings / X-Rays See fee schedule Covered 100%
Basic Services: Covered 100%
Fillings / Root Canal / Oral Surgery See fee schedule
Major Services: 30% coinsurance
Crowns / Dentures / See fee schedule
Orthodontia $2,000 child 50% up to $1,500 lifetime max
$2,000 adult (child & adult)
Please refer to carrier benefit summaries for more detailed information & out-of-network benefits.
On the PPO plan Out of Network services are covered up to the 90 percentile of reasonable & customary.
th
** On DPPO deductible applies to Basic & Major services. See Benefit Summary.
DHMO Dental is not available in ALL STATES. You must elect a primary care Dentist. Find providers link below:
change zip code based off your location preference
VSP Vision Plan
In- Network (VSP Signature) Out-of-Network
Exam & Materials $20 Combined Copay Up to $50
(once every 12 months)
Lenses- Single, Bifocal, Trifocal Covered in full after copay Up to $50 / $75 / $100
(once every 12 months)
Frames $130 allowance + 20% off
remaining balance Up to $70
Additional Frames $70 Walmart/Costco allowance
(once every 12 months) $150 allowance featured frame brands
Contact Lenses – elective* $130 allowance Up to $105
(once every 12 months)
Contact Lenses – non-elective Covered in full Up to $210
(once every 12 months)
*Elective Contact Lenses (in lieu of frames & lenses)
For additional vision benefits see benefit summary.
Find Providers on link below:
https://www.vsp.com/eye-doctor
PAGE 6