
Page 3 - Magnet Employee Benefits Brochure 2021-22 FINAL
P. 3
2021–2022 Employee Benefits Brochure
Medical Plan
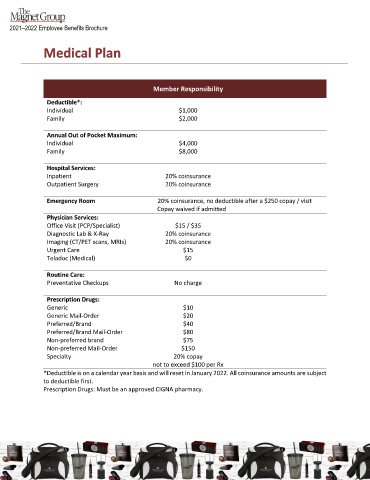
Member Responsibility
Deductible*:
Individual $1,000
Family $2,000
Annual Out of Pocket Maximum:
Individual $4,000
Family $8,000
Hospital Services:
Inpatient 20% coinsurance
Outpatient Surgery 20% coinsurance
Emergency Room 20% coinsurance, no deductible after a $250 copay / visit
Copay waived if admitted
Physician Services:
Office Visit (PCP/Specialist) $15 / $35
Diagnostic Lab & X-Ray 20% coinsurance
Imaging (CT/PET scans, MRIs) 20% coinsurance
Urgent Care $15
Teladoc (Medical) $0
Routine Care:
Preventative Checkups No charge
Prescription Drugs:
Generic $10
Generic Mail-Order $20
Preferred/Brand $40
Preferred/Brand Mail-Order $80
Non-preferred brand $75
Non-preferred Mail-Order $150
Specialty 20% copay
not to exceed $100 per Rx
*Deductible is on a calendar year basis and will reset in January 2022. All coinsurance amounts are subject
to deductible first.
Prescription Drugs: Must be an approved CIGNA pharmacy.
PAGE 2