
Page 10 - 2021 Sample Benefit Booklet
P. 10
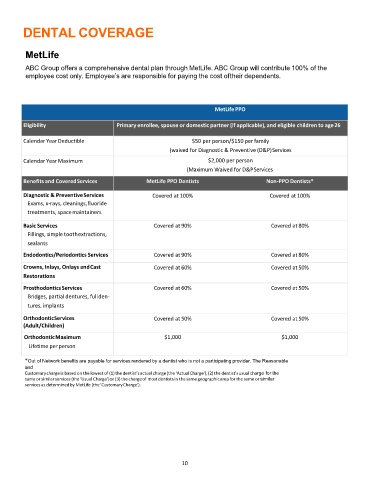
DENTAL COVERAGE
MetLife
ABC Group offers a comprehensive dental plan through MetLife. ABC Group will contribute 100% of the
employee cost only. Employee’s are responsible for paying the cost oftheir dependents.
MetLife PPO
Eligibility Primary enrollee, spouse or domestic partner (if applicable), and eligible children to age26
Calendar Year Deductible $50 per person/$150 per family
(waived for Diagnostic & Preventive (D&P)Services
Calendar Year Maximum $2,000 per person
(Maximum Waived for D&PServices
Benefits and CoveredServices MetLife PPO Dentists Non‐PPO Dentists*
Diagnostic & PreventiveServices Covered at 100% Covered at 100%
Exams, x‐rays, cleanings,fluoride
treatments, spacemaintainers
Basic Services Covered at 90% Covered at 80%
Fillings, simple toothextractions,
sealants
Endodontics/Periodontics Services Covered at 90% Covered at 80%
Crowns, Inlays, Onlays andCast Covered at 60% Covered at 50%
Restorations
ProsthodonticsServices Covered at 60% Covered at 50%
Bridges, partial dentures, fullden‐
tures, implants
OrthodonticServices Covered at 50% Covered at 50%
(Adult/Children)
OrthodonticMaximum $1,000 $1,000
Lifetime perperson
*Out of Network benefits are payable for services rendered by a dentist who is not a participating provider. The Reasonable
and
Customarychargeis based on the lowest of (1)the dentist’sactual charge(the ‘ActualCharge’),(2)the dentist’susual charge for the
same or similarservices (the ‘UsualCharge’)or (3)the chargeof mostdentistsin the same geographicarea for the same or similar
servicesas determinedby MetLife (the‘CustomaryCharge’).
10